
Table of Contents
Introduction
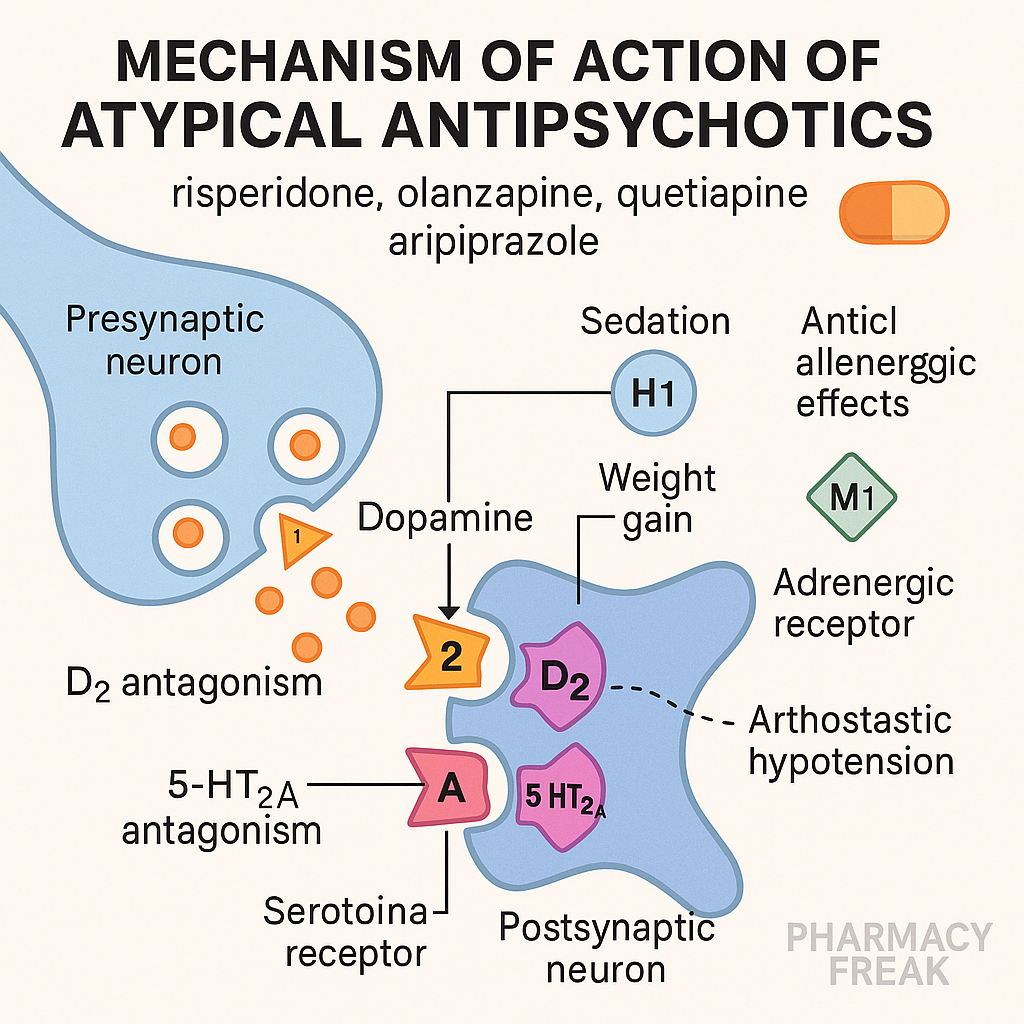
Atypical antipsychotics, also known as second-generation antipsychotics (SGAs), are widely used in the treatment of schizophrenia, bipolar disorder, major depressive disorder (as adjuncts), and autism-related irritability. Compared to typical antipsychotics, they offer fewer extrapyramidal symptoms (EPS) and better control of negative symptoms of schizophrenia due to their dual action on dopamine and serotonin receptors.
Common SGAs include:
- Clozapine
- Risperidone
- Olanzapine
- Quetiapine
- Aripiprazole
- Ziprasidone
- Lurasidone
Stepwise Mechanism of Action of Atypical Antipsychotics
- Dopamine D2 receptor antagonism (weaker than typicals)
SGAs block dopamine D2 receptors, but with lower affinity, particularly in the mesolimbic pathway, which reduces positive symptoms of schizophrenia. - Serotonin 5-HT2A receptor antagonism
SGAs strongly block 5-HT2A receptors, especially in the mesocortical pathway, which improves negative and cognitive symptoms and reduces EPS. - Modulation of dopamine release
By blocking 5-HT2A receptors, SGAs indirectly increase dopamine release in the nigrostriatal pathway, reducing the risk of motor side effects. - Partial agonism (e.g., aripiprazole)
Some SGAs like aripiprazole act as partial D2 agonists, balancing dopamine activity rather than completely blocking it. - Additional receptor interactions
Many SGAs also block H1, alpha-1, and muscarinic receptors, contributing to sedation, orthostatic hypotension, and anticholinergic effects.


Pharmacokinetic Parameters of Atypical Antipsychotics
| Drug | Half-life | Metabolism | Unique Feature |
|---|---|---|---|
| Clozapine | 8–12 hrs | CYP1A2 | Agranulocytosis risk; best for treatment-resistant cases |
| Risperidone | 20 hrs | CYP2D6 | Causes dose-dependent EPS and prolactin increase |
| Olanzapine | 20–54 hrs | CYP1A2 | High risk of weight gain and metabolic syndrome |
| Quetiapine | 6–7 hrs | CYP3A4 | Sedating; low EPS risk |
| Aripiprazole | 75 hrs | CYP2D6, 3A4 | Partial D2 agonist; minimal weight gain |
| Ziprasidone | 7 hrs | CYP3A4 | Low metabolic risk, QT prolongation risk |
| Lurasidone | 18 hrs | CYP3A4 | Fewer metabolic effects, requires food for absorption |
Clinical Uses of Atypical Antipsychotics
- Schizophrenia (positive and negative symptoms)
- Bipolar disorder (mania, depression, maintenance)
- Major depressive disorder (adjunctive)
- Autism-related irritability
- Tourette syndrome
- Treatment-resistant schizophrenia (clozapine)
Adverse Effects of Atypical Antipsychotics
- Metabolic syndrome – weight gain, hyperlipidemia, insulin resistance (especially olanzapine, clozapine)
- Sedation (H1 blockade)
- Orthostatic hypotension (alpha-1 blockade)
- Hyperprolactinemia (risperidone, paliperidone)
- QT prolongation (ziprasidone)
- Agranulocytosis (clozapine – requires CBC monitoring)
- Seizures (dose-dependent with clozapine)
- Minimal EPS (except risperidone at higher doses)
Comparative Analysis: Atypical vs Typical Antipsychotics
| Feature | Atypical Antipsychotics | Typical Antipsychotics |
|---|---|---|
| D2 receptor binding | Moderate | High affinity |
| 5-HT2A blockade | Strong | Minimal |
| EPS risk | Lower | Higher |
| Effect on negative symptoms | Better | Minimal or worsens |
| Weight gain/metabolic risk | Higher in some | Lower |
| Prolactin elevation | Variable (high with risperidone) | High |
Practice MCQs
Q1. Atypical antipsychotics differ from typicals mainly by blocking:
a. D1 receptors
b. 5-HT1A receptors
c. 5-HT2A receptors ✅
d. NMDA receptors
Q2. Which atypical antipsychotic causes agranulocytosis?
a. Risperidone
b. Clozapine ✅
c. Olanzapine
d. Ziprasidone
Q3. Which SGA has minimal weight gain?
a. Olanzapine
b. Aripiprazole ✅
c. Clozapine
d. Quetiapine
Q4. SGAs reduce EPS because of:
a. D1 antagonism
b. Partial 5-HT1A agonism
c. 5-HT2A antagonism ✅
d. Alpha-2 blockade
Q5. Which SGA is approved for treatment-resistant schizophrenia?
a. Risperidone
b. Quetiapine
c. Clozapine ✅
d. Aripiprazole
Q6. What is the MOA of aripiprazole?
a. Full D2 antagonist
b. D2 partial agonist ✅
c. Serotonin agonist
d. NMDA blocker
Q7. Metabolic syndrome is most associated with:
a. Lurasidone
b. Olanzapine ✅
c. Ziprasidone
d. Aripiprazole
Q8. Which SGA prolongs QT interval the most?
a. Risperidone
b. Ziprasidone ✅
c. Quetiapine
d. Aripiprazole
Q9. What blood test is mandatory for clozapine use?
a. LFTs
b. Lipid profile
c. CBC ✅
d. RFTs
Q10. Why are SGAs preferred over FGAs?
a. Faster onset
b. Better for hallucinations
c. Fewer motor side effects ✅
d. Cheaper
FAQs
Q1: Do SGAs treat both positive and negative symptoms of schizophrenia?
Yes, they are effective against both symptom domains, especially due to 5-HT2A blockade.
Q2: Why is clozapine rarely used despite its efficacy?
Due to risks of agranulocytosis, seizures, and myocarditis, requiring close monitoring.
Q3: Can SGAs be used in children?
Yes. Some like risperidone and aripiprazole are FDA-approved for pediatric use.
Q4: Which SGA causes the most weight gain?
Olanzapine, followed by clozapine.
Q5: What is a unique feature of aripiprazole?
It is a partial D2 receptor agonist, reducing both positive and negative symptoms with fewer side effects.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK519489/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com