

Table of Contents
Introduction
Lithium is the gold-standard mood stabilizer, used for managing bipolar disorder, especially to control acute manic episodes and prevent future mood swings. Though its exact mechanism isn’t completely understood, it’s known to influence intracellular signaling, neurotransmitter modulation, and second messenger systems. Lithium is also one of the few psychiatric medications that significantly reduces suicide risk.
It’s a high-yield drug in exams like USMLE, NCLEX, GPAT, and NEET-PG.

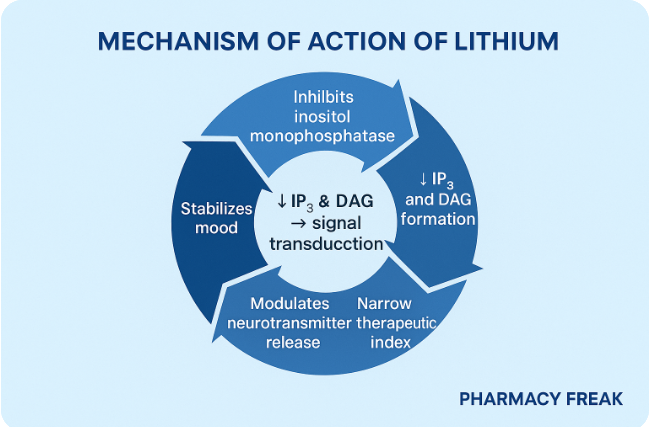
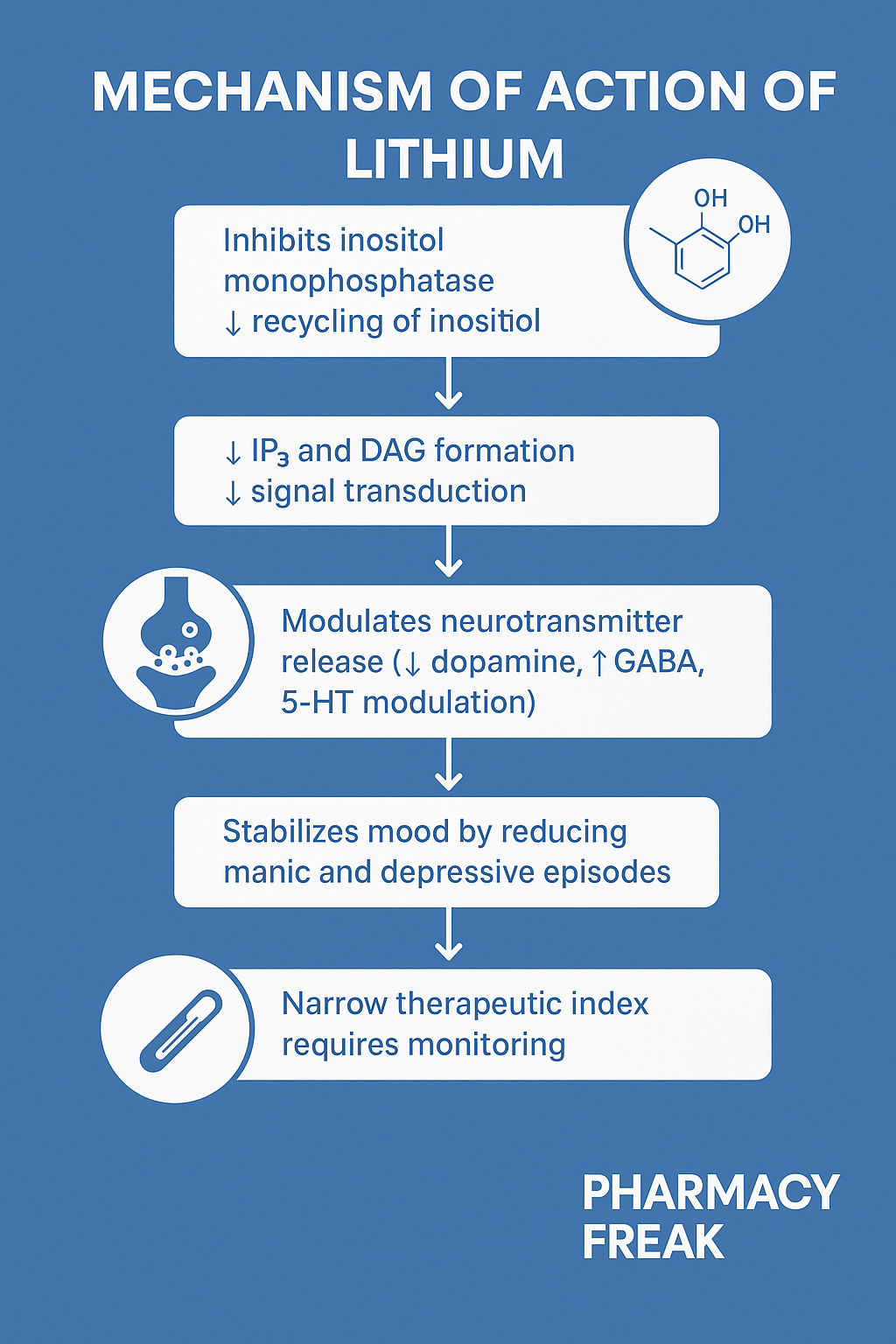
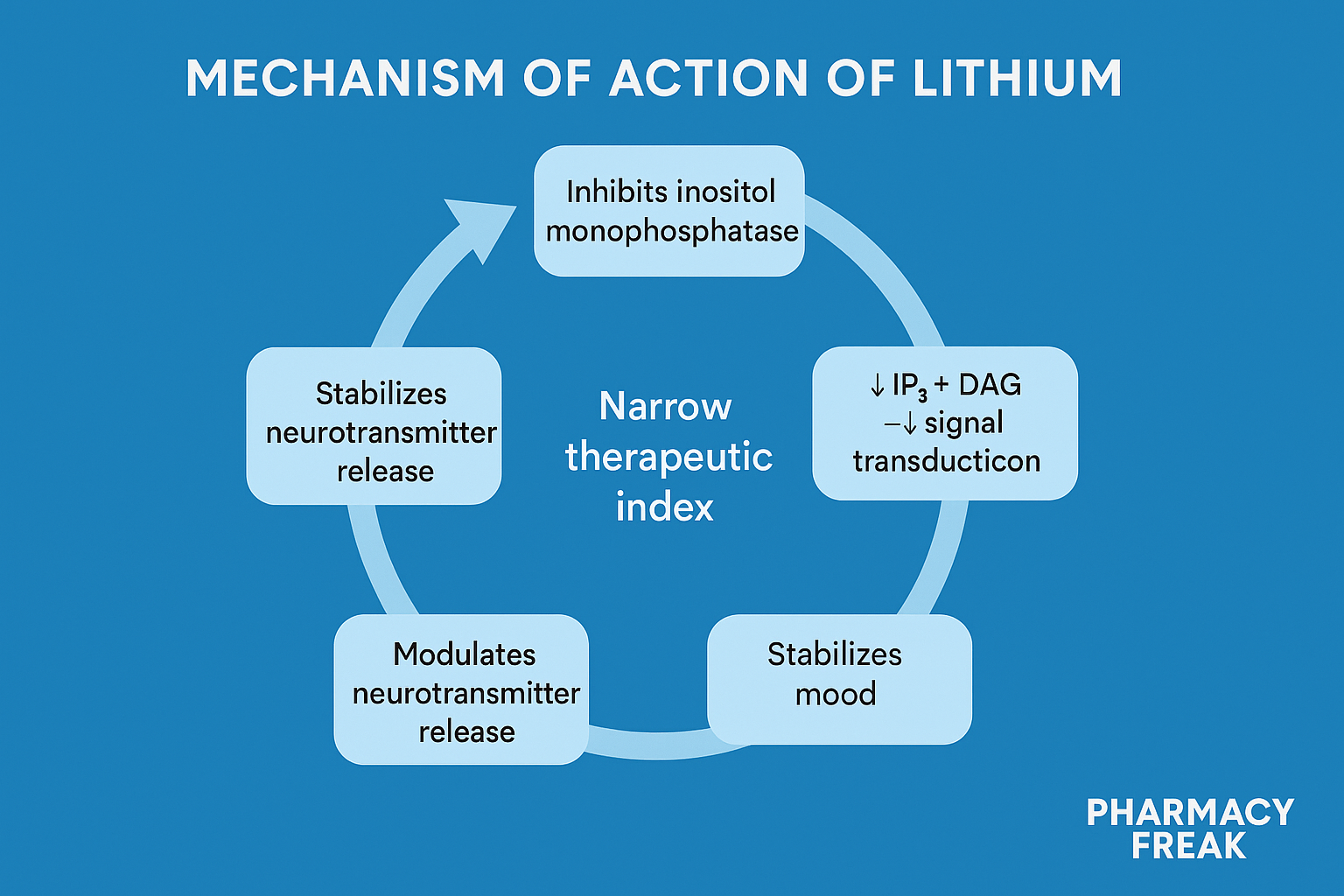
Stepwise Mechanism of Action of Lithium
- Inhibition of inositol monophosphatase
Lithium inhibits inositol monophosphatase, preventing the regeneration of free inositol, a key component in the phosphatidylinositol (PI) second messenger system. - Reduced IP3 and DAG production
This leads to reduced levels of IP3 and DAG, important for signal transduction of various neurotransmitters like norepinephrine and serotonin. - Inhibition of glycogen synthase kinase-3 (GSK-3)
Lithium inhibits GSK-3, an enzyme that plays a role in cell apoptosis, circadian rhythm, and neuroplasticity. This may help stabilize mood. - Modulation of neurotransmitters
Lithium is believed to enhance serotonergic activity, reduce dopaminergic overactivity, and stabilize glutamate levels in the brain. - Neuroprotective effects
Lithium may promote neuronal survival and neurogenesis, contributing to its long-term mood-stabilizing action.


Pharmacokinetic Parameters of Lithium
| Parameter | Value |
|---|---|
| Bioavailability | 95–100% |
| Onset of action | 5–7 days for antimanic effect |
| Half-life | 18–36 hours (longer in elderly) |
| Metabolism | Not metabolized (excreted unchanged) |
| Excretion | Renal – >95% via glomerular filtration |
| Therapeutic range | 0.6–1.2 mEq/L (narrow therapeutic index) |
Clinical Uses of Lithium
- Bipolar disorder (acute mania and maintenance)
- Schizoaffective disorder
- Augmentation in refractory depression
- Cluster headaches (off-label)
- Suicide prevention in mood disorders
Adverse Effects of Lithium
- Tremor
- Hypothyroidism (inhibits thyroid hormone synthesis)
- Nephrogenic diabetes insipidus (polyuria, polydipsia)
- Weight gain
- GI upset (nausea, diarrhea)
- Leukocytosis
- Teratogenicity – causes Ebstein’s anomaly (if taken during 1st trimester)
- Toxicity – confusion, ataxia, seizures, coma (esp. with NSAIDs, diuretics)
Comparative Analysis: Lithium vs Valproate (Another Mood Stabilizer)
| Feature | Lithium | Valproate |
|---|---|---|
| Onset of action | Slow (5–7 days) | Faster (2–4 days) |
| Metabolism | Not metabolized (renal excretion) | Hepatic metabolism |
| Teratogenicity | Ebstein anomaly | Neural tube defects |
| Use in rapid cycling | Less effective | More effective |
| Therapeutic range | Narrow | Moderate |
Practice MCQs
Q1. Lithium primarily inhibits which enzyme?
a. Tyrosine hydroxylase
b. Monoamine oxidase
c. Inositol monophosphatase ✅
d. COMT
Q2. Lithium is most effective in:
a. Acute psychosis
b. Bipolar mania ✅
c. OCD
d. PTSD
Q3. Which organ excretes lithium?
a. Liver
b. Kidney ✅
c. Lungs
d. Pancreas
Q4. Lithium toxicity risk increases with:
a. ACE inhibitors
b. Diuretics
c. NSAIDs
d. All of the above ✅
Q5. Which cardiac defect is linked to lithium use in pregnancy?
a. Tetralogy of Fallot
b. ASD
c. Ebstein anomaly ✅
d. PDA
Q6. Lithium can cause:
a. Hyperthyroidism
b. Hypothyroidism ✅
c. Hyperparathyroidism
d. Pheochromocytoma
Q7. Which is NOT a known side effect of lithium?
a. Tremor
b. Leukopenia ✅
c. Weight gain
d. Polyuria
Q8. Lithium is most dangerous when combined with:
a. Paracetamol
b. Metoprolol
c. NSAIDs ✅
d. SSRIs
Q9. What is the therapeutic plasma range for lithium?
a. 0.2–0.6 mEq/L
b. 0.6–1.2 mEq/L ✅
c. 1.5–2.5 mEq/L
d. 2.5–3.5 mEq/L
Q10. Neuroprotective action of lithium is partly due to:
a. GABA enhancement
b. Inhibition of GSK-3 ✅
c. MAO inhibition
d. NMDA blockade
FAQs
Q1: How long does lithium take to work?
It usually takes 5–7 days for antimanic effects to begin.
Q2: Is lithium safe during pregnancy?
No. It’s teratogenic, especially in the first trimester.
Q3: What tests are needed during lithium therapy?
Monitor serum lithium levels, renal function, thyroid function, and electrolytes regularly.
Q4: What happens in lithium toxicity?
Symptoms include tremor, confusion, ataxia, seizures, and coma.
Q5: Can lithium be used long-term?
Yes, but requires strict monitoring due to narrow therapeutic index and renal risks.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Sparsh Gupta – Review of Pharmacology
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK526101/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com