Table of Contents
Introduction
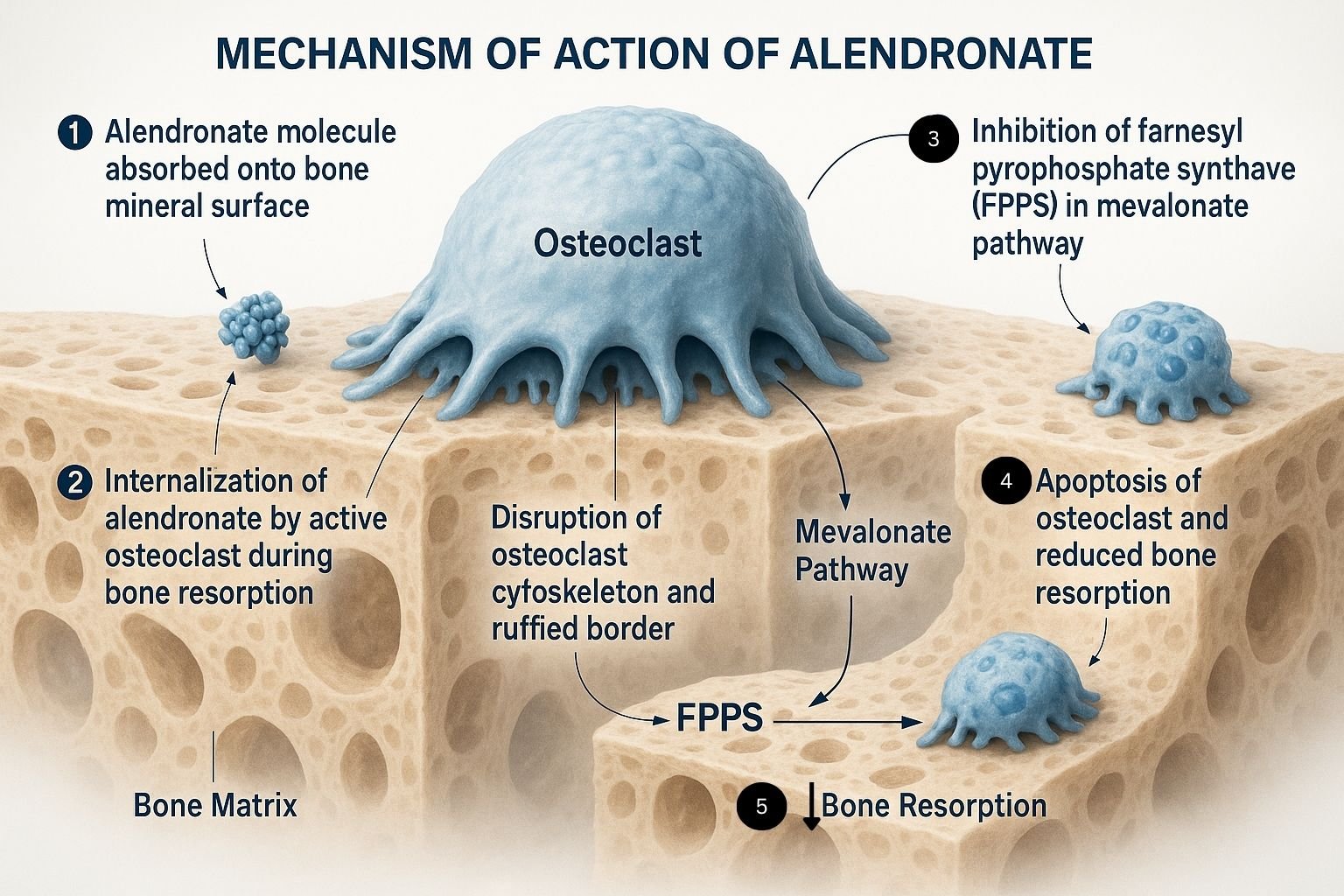
Alendronate is a nitrogen-containing bisphosphonate used primarily in the treatment and prevention of osteoporosis and other bone-resorptive disorders. It acts by inhibiting osteoclast-mediated bone resorption, thereby maintaining or increasing bone mineral density.
Mechanism of Action (Stepwise Points)

- Bone Affinity
Alendronate has a strong affinity for hydroxyapatite in bone, particularly at sites of active resorption. - Osteoclast Uptake
During bone resorption, osteoclasts internalize alendronate from the bone matrix. - Inhibition of Farnesyl Pyrophosphate Synthase (FPPS)
Alendronate inhibits the mevalonate pathway enzyme FPPS, crucial for prenylation of small GTPase signaling proteins. - Osteoclast Dysfunction and Apoptosis
Inhibition of prenylation disrupts cytoskeletal organization and vesicular trafficking in osteoclasts, leading to loss of function and apoptosis. - Reduced Bone Resorption
These effects cumulatively decrease bone turnover and maintain bone strength.


Pharmacokinetics
- Absorption: Poor oral bioavailability (~0.6%); significantly reduced by food or beverages other than plain water.
- Distribution: Rapidly binds to bone; unbound drug is cleared rapidly.
- Metabolism: Not metabolized.
- Excretion: Primarily excreted unchanged in urine.
- Half-life: Long terminal half-life (>10 years) due to skeletal retention.
Clinical Uses
- Osteoporosis (postmenopausal, male, glucocorticoid-induced)
- Paget’s disease of bone
- Osteogenesis imperfecta (off-label)
- Hypercalcemia of malignancy (alternative bisphosphonates preferred)
Adverse Effects
- Esophagitis and esophageal ulcers (especially if not taken properly)
- Musculoskeletal pain
- Hypocalcemia
- Atypical femur fractures (with prolonged use)
- Osteonecrosis of the jaw (rare)
- Abdominal discomfort, flatulence
Comparative Analysis
| Parameter | Alendronate | Risedronate | Zoledronate |
|---|---|---|---|
| Route | Oral | Oral | IV |
| Dosing Frequency | Weekly | Weekly or monthly | Once yearly |
| GI Side Effects | More common | Moderate | Minimal |
| Onset of Action | Gradual | Gradual | Rapid |
| Renal Clearance | Yes | Yes | Yes |
Explanation: Alendronate offers a convenient oral dosing schedule but requires adherence to administration protocols to minimize GI complications. Zoledronate, though IV, is preferred for those with compliance or GI issues.
Multiple Choice Questions (MCQs)
- What is the primary molecular target of alendronate?
a) COX-2
b) Parathyroid hormone receptor
c) Farnesyl pyrophosphate synthase
d) Calcitonin receptor - How should alendronate be taken for optimal absorption?
a) With food
b) After breakfast
c) On an empty stomach with plain water
d) With milk - The long half-life of alendronate is due to its:
a) Hepatic metabolism
b) Bone binding and skeletal retention
c) Enterohepatic circulation
d) Plasma protein binding - Which adverse effect is specifically associated with bisphosphonates like alendronate?
a) Hepatotoxicity
b) Esophagitis
c) Weight gain
d) Arrhythmias - Which of the following is a contraindication for oral alendronate?
a) Osteoporosis
b) Renal stones
c) Esophageal stricture
d) Arthritis - Alendronate is NOT effective in:
a) Osteoporosis
b) Paget’s disease
c) Glucocorticoid-induced bone loss
d) Osteoarthritis - Alendronate causes apoptosis in which cell type?
a) Osteoblasts
b) Osteoclasts
c) Chondrocytes
d) Fibroblasts - What class of drug is alendronate?
a) Calcitonin analog
b) Bisphosphonate
c) Selective estrogen receptor modulator
d) PTH analog - Which condition requires caution with alendronate therapy?
a) Hypertension
b) Chronic kidney disease
c) Diabetes mellitus
d) Hyperlipidemia - Osteonecrosis of the jaw is associated with prolonged use of:
a) Teriparatide
b) Calcitonin
c) Alendronate
d) Raloxifene
FAQs
Q1: Why should alendronate be taken with water and remain upright after?
A1: To prevent esophageal irritation or ulceration.
Q2: Can alendronate be used in men?
A2: Yes, for osteoporosis and secondary prevention of fractures.
Q3: Is alendronate suitable for renal impairment?
A3: Use with caution; contraindicated if creatinine clearance <35 mL/min.
Q4: How long should alendronate therapy continue?
A4: Typically 3–5 years, then reassessed due to risk of long-term skeletal side effects.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 12th Edition
- KD Tripathi, Essentials of Medical Pharmacology, 7th Edition
- Pharmacological Screening Methods & Toxicology by Avanapu Srinivasa Rao
- Biopharmaceutics & Pharmacokinetics by Thakur Publication
