
There are many natural substances of vegetable, animal, and mineral origin. These substances are mostly beneficial but some are even harmful to mankind if not used properly and are misused. Morphine and allied alkaloids of opium, cocaine, coca leaves, cannabinoids, and other resins of Cannabis indica, ergot, etc. are examples of such drugs. These are added substances of synthetic organic chemistry origin, like heroin and pethidine that produce harmful effects.
These drugs unnecessarily depress or stimulate the human brain and also produce euphoria, personality destabilizing effects, addiction, etc. These drugs are termed narcotics and to exercise control over their use, the International level convention was held in 1919 in Geneva. After that, many other conventions were organized. Before India gained independence, the Dangerous Drugs Act was passed in 1930.
Different states have framed their own rules for the implementation of this Act. As per the laws of this Act, the cultivation, possession, transport, dispensing, distribution, and administration of opium, Indian hemp, and coca are regulated and controlled. This law however did not cover synthetic and semi-synthetic products, like pethidine, L.S.D., etc., which were not yet identified at that time. These aspects of sale and possession by retailers, etc., are now covered by schedules H, L, and X of the Drugs and Cosmetics Act, of 1940. In the Rules 1945, drugs other than opium, coca, and Indian hemp which are covered by Schedule H and cannot be sold except against a prescription of the registered medical practitioner are included. Drugs causing addiction, like opium, coca, etc., are included in Schedule X.
Hospital Control Procedures
The American government authorities have evolved the procedure given below and applies to Indian hospitals:
Responsibility for Controlled Substances in the Hospital
The administrative head of the hospital properly safeguards and handles the controlled substances in the hospital. The Medical Superintendent or Dean is the administrative head of Indian hospitals. The Chief Pharmacist (in the U.S.A.) or the medical officer (in India) looks after the purchase, storage, accountability, and proper dispensing of bulk controlled substances in the hospital. The Matron or Head Nurse looks after the proper storage and use of the controlled substances in the nursing unit.
Ordering Ward Stock of Controlled Substances from the Pharmacy
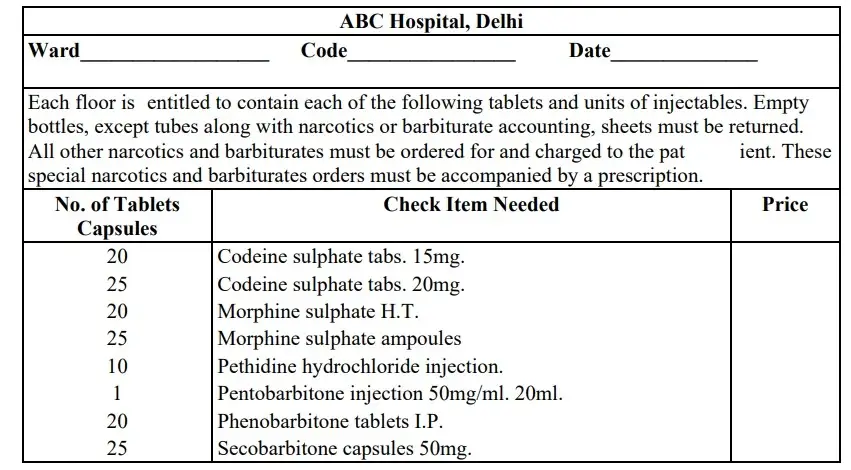
The procedure given below is followed while ordering controlled substances from the ward stock of the pharmacy.
- By placing a checkmark (✓) in front of the name and desired strength of the controlled substance, the requisition forward stock controlled substances is completed. This form along with the empty containers and the nurses‟ inventory sheet is then forwarded to the pharmacy.
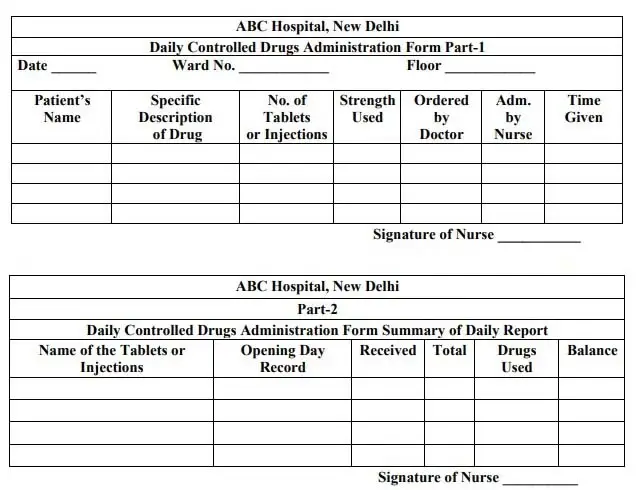
- Before issuing any new controlled substances to a ward, the previous supply should be fully looked into. Therefore, the request for every new supply should be accompanied by the daily controlled substances.
Ordering Non-Ward Stock Controlled Drugs from Pharmacy
Drugs not stocked at the nursing stations are ordered from the pharmacy through written prescriptions. Only the amount of drugs stated on the prescription by the physician’s signature should be sent to the nursing unit. If an additional amount is required, a new signed prescription should be obtained. Such a prescription should carry the following information:
- Patient’s full name
- Patient’s hospital number or address
- Date
- Name and strength of the prescribed drug
- Quantity of the drug to be dispensed
- Physician’s registration number
The prescription should be written properly with no cuttings or alterations using ink or permanent pencil. A physician cannot prescribe controlled drugs for his use.
Prescribing Controlled Drugs in the Out-Patient Department
The prescription for narcotic drugs under the Narcotics and Psychotropic Substances Act, 1985, and those covered by schedule X to be dispensed from the out-patient pharmacy should bear the following information:
- Patient’s full name
- Patient’s hospital number or address
- Date
- Name and strength of the prescribed drug
- Quantity of the drug to be dispensed
- Frequency and route of administration
- Physician’s signature.
The prescription should be written properly with no cuttings or alterations using ink or permanent pencil.
Dispensing Controlled Drugs for Home Use when the Pharmacy is Closed
Sometimes, patients are discharged from the hospitals during hours when the hospital pharmacy is closed and are prescribed controlled drugs for home use. In such cases, a prescription should be signed by a registered medical practitioner, who is also authorized to prescribe narcotics and other controlled drugs. A physician authorized to prescribe controlled drugs should write on the prescription blank. If this is not available, he/she should mention the office address on the hospital prescription blank so that the patients or their relatives can purchase the
drugs from an outside pharmacy. This could be followed if a physician is unavailable or even if the local pharmacies are closed; however, this should be done only in an emergency. The attending physician will calculate the smallest amount of narcotic drug required for the patient at that moment until the pharmacy opens. He/she will prescribe this amount and the nurse dispenses the medication from her stock supply. The next day when the pharmacy opens, this prescription should be presented to the pharmacy for stock replacement.
Procedure in Case of Waste, Destruction, Contamination, etc.
- Aliquot Part of Narcotic Solution Unused: The nurse should use a proper number of tablets or ampoules from the nursing stock. She should keep a record of the number of tablets or ampoules used and the dose given in proper columns on the daily Controlled Drugs Administration Form. On attaining the proper aliquot part, the portion of the solution that is not used should be discarded into the sink by the nurse.
- Prepared Dose Refused by Patient or Cancelled by Doctor: When a dose has been prepared but is left unused in case the patient refuses to take it in or the physician cancels the dose, the nurse should discard the solution into the sink and record the reason for drug not being administered. For example, “Discarded refused by patient or order canceled by Doctor”. The head nurse of the nursing unit should countersign this statement.
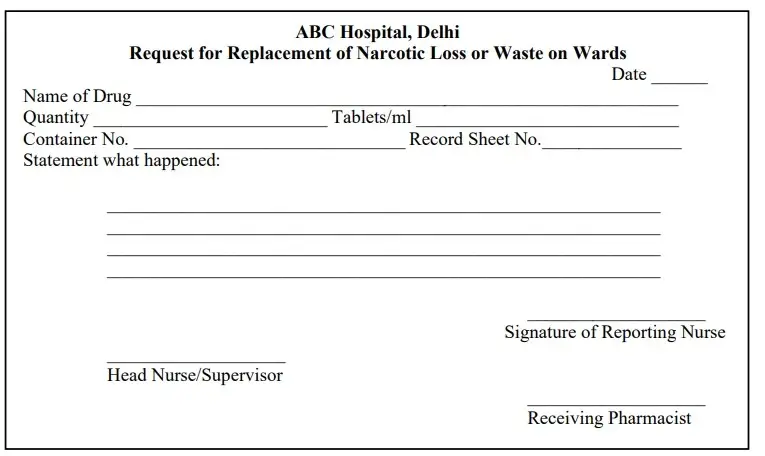
- Accidental Destruction or Contamination of Drugs: If any solution, ampoules, tablets, etc., gets accidentally destroyed or contaminated in a nursing unit, the responsible person should indicate the loss.
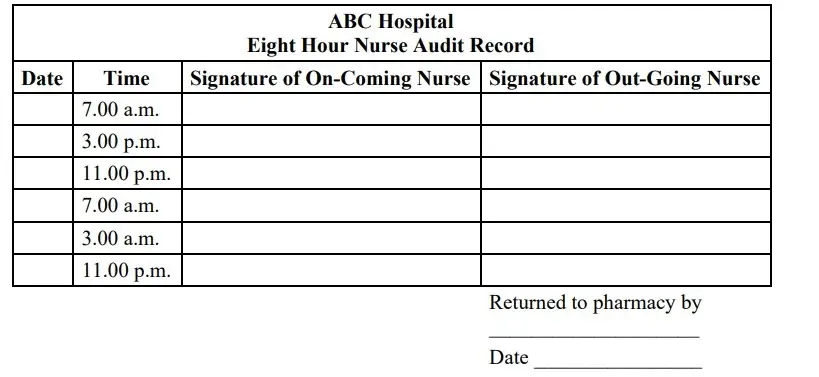
- Control of Narcotics on the Ward by Nurses: When the pharmacy has dispensed the narcotics for the ward, the nursing service assumes the responsibility for administration, control, and auditing of the inventory. The auditing of narcotic inventory takes place with each charge of the nursing shift. At this time, the nurse coming on duty as well as the nurse going off-duty -duty physically counts the narcotics at the nursing station.The audit record is signed by both of them if the tally is correct. In case the tally is not correct, the medications ordered on that day by the physician are re-checked to immediately amend the recording error. If the error cannot be explained, the narcotic loss report should be forwarded to the pharmacy department.
Narcotics-Delivery to the Ward
The narcotics from the pharmacy should be delivered to the ward and nursing station by a reliable individual working in the hospital. This responsibility is mainly given to a member of the messenger staff. Sufficient control records are maintained to detect illegal delivery of any narcotics and to take necessary steps for their recovery.
Charges for Narcotic to Patients
Charges for narcotics depend on the policy of each hospital. The general pattern of charging is as follows:
- Charges are made for each dose received.
- A flat charge is made for all narcotics and hypnotics. Hospitals include narcotics alone with other floor-stock drugs for which the patient is not specifically charged.
- In hospitals having a „split‟ policy, the patient is not charged for narcotics used routinely but is charged for those obtained on special order.
Related Articles

