Table of Contents
Introduction
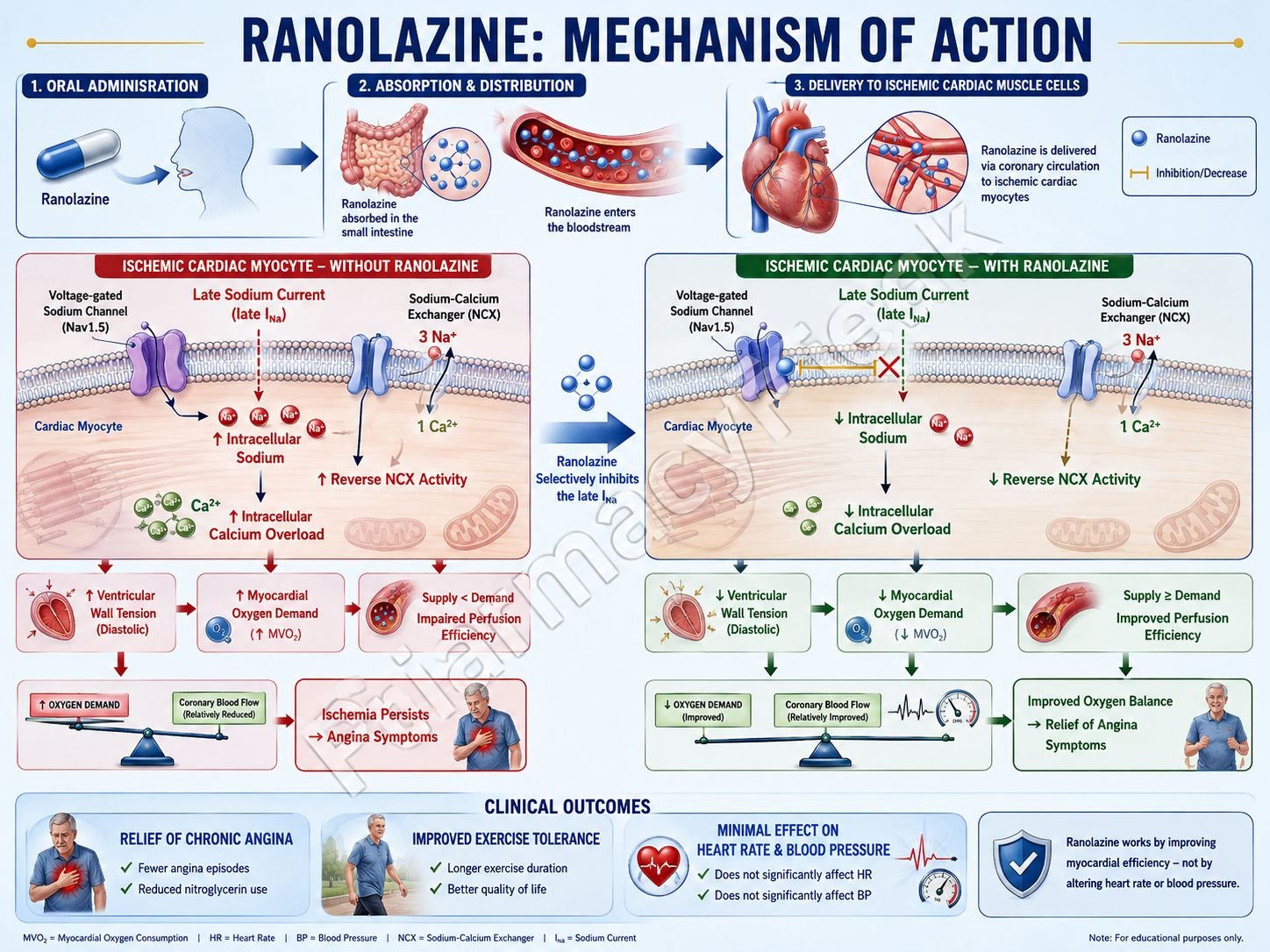
Ranolazine is an antianginal medication primarily used in the treatment of chronic stable angina. Unlike traditional antianginal drugs, it has minimal effects on heart rate and blood pressure. Ranolazine improves myocardial efficiency and reduces ischemia mainly by inhibiting abnormal sodium influx in cardiac cells.
Mechanism of Action (Step-wise)
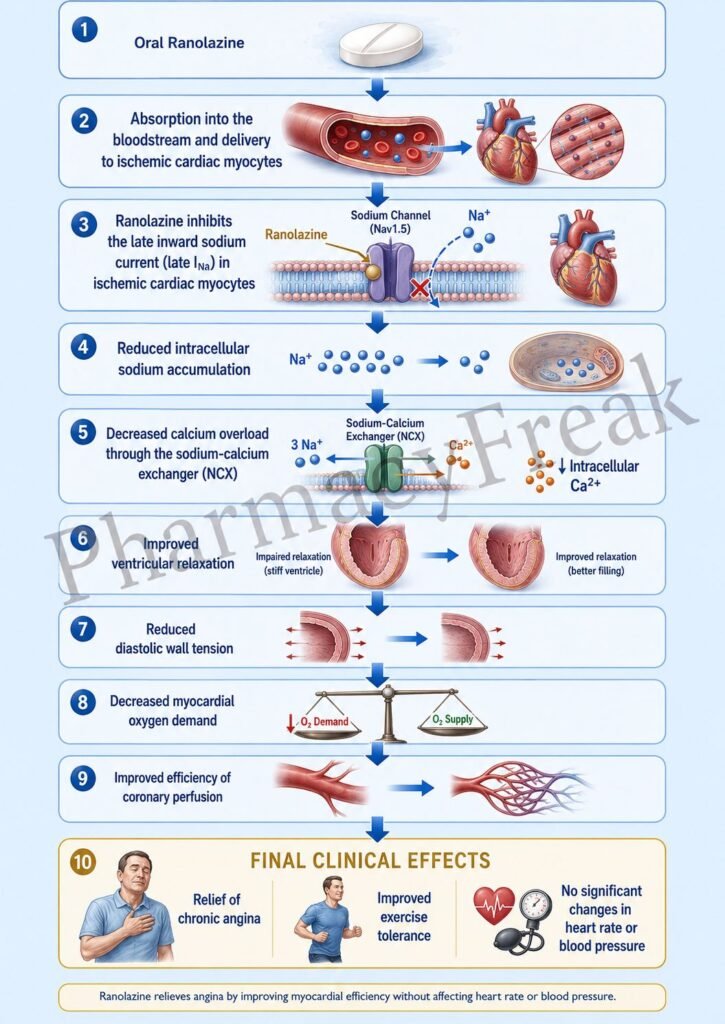
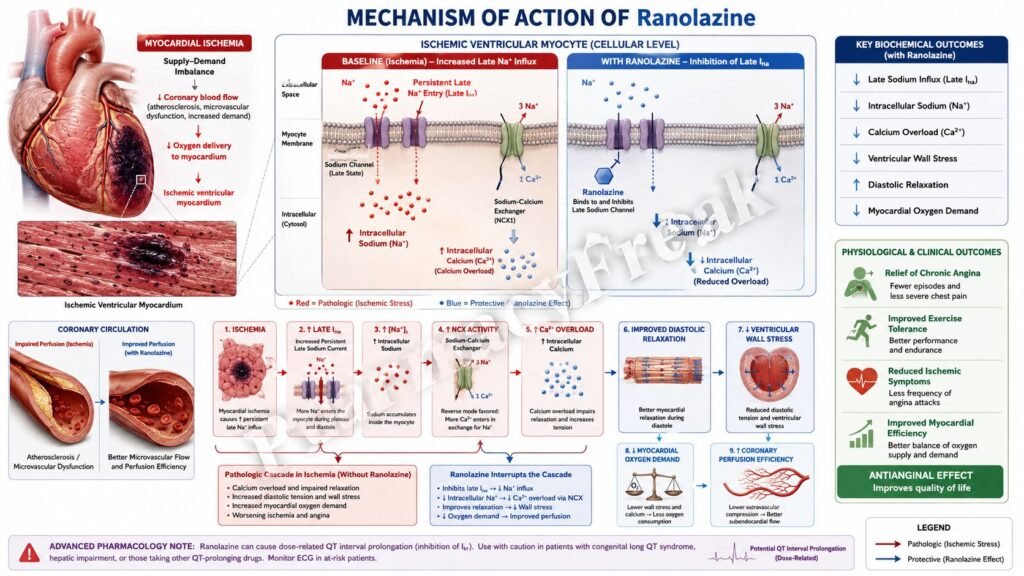
- During myocardial ischemia, late inward sodium current (late INa) in cardiac myocytes increases abnormally.
- Excess sodium accumulates inside cardiac cells.
- Increased intracellular sodium alters the sodium-calcium exchanger (NCX).
- Reduced calcium extrusion causes intracellular calcium overload.
- Excess intracellular calcium increases ventricular wall tension and myocardial oxygen consumption.
- Ranolazine selectively inhibits the late sodium current in cardiac myocytes.
- Reduced sodium influx lowers intracellular sodium concentration.
- Improved sodium-calcium exchange decreases intracellular calcium overload.
- Reduced calcium levels improve myocardial relaxation during diastole.
- Ventricular wall tension and oxygen demand decrease.
- Coronary perfusion during diastole improves.
- The overall effect is reduction of myocardial ischemia and anginal symptoms without major changes in heart rate or blood pressure.
A key exam point is that ranolazine inhibits the late sodium current in ischemic cardiac cells, reducing intracellular calcium overload.
Pharmacokinetics
Ranolazine is administered orally and is well absorbed. It undergoes hepatic metabolism mainly through CYP3A4 and partially through CYP2D6. The drug has an extended-release formulation commonly used for chronic therapy. Elimination occurs through both renal and fecal routes.
Clinical Uses
Ranolazine is used in chronic stable angina, especially in patients who remain symptomatic despite standard therapy or who cannot tolerate reductions in blood pressure or heart rate caused by other antianginal drugs.
Adverse Effects
Common adverse effects include dizziness, headache, constipation, and nausea. Ranolazine may prolong the QT interval and should be used cautiously in patients with arrhythmia risk. Drug interactions may occur with CYP3A4 inhibitors.
Comparative Analysis
| Feature | Ranolazine | Nitroglycerin | Metoprolol |
|---|---|---|---|
| Main mechanism | Late Na⁺ current inhibition | Nitric oxide-mediated vasodilation | β1 blockade |
| Effect on heart rate | Minimal | Reflex increase possible | Decreases |
| Effect on blood pressure | Minimal | Decreases | Decreases |
| Main use | Chronic stable angina | Acute angina relief | Angina and hypertension |
| QT prolongation risk | Present | Minimal | Minimal |
| Oxygen demand reduction | Indirect | Direct | Direct |
Ranolazine differs from nitroglycerin and β blockers because it improves myocardial metabolism and relaxation without major hemodynamic effects.
MCQs
- Ranolazine is mainly used to treat:
a) Asthma
b) Chronic stable angina
c) Epilepsy
d) Hyperthyroidism
Answer: b) Chronic stable angina
- Ranolazine primarily inhibits:
a) Calcium channels
b) Late sodium current
c) Potassium channels only
d) β receptors
Answer: b) Late sodium current
- Increased late sodium current during ischemia causes accumulation of:
a) Chloride
b) Intracellular sodium
c) Magnesium
d) Histamine
Answer: b) Intracellular sodium
- Excess intracellular sodium indirectly increases intracellular:
a) Potassium
b) Calcium
c) Chloride
d) Phosphate
Answer: b) Calcium
- Ranolazine improves myocardial:
a) Contraction only
b) Relaxation during diastole
c) Valve function
d) Pacemaker automaticity only
Answer: b) Relaxation during diastole
- Ranolazine decreases myocardial:
a) Oxygen demand
b) Calcium excretion
c) Sodium intake
d) Histamine release
Answer: a) Oxygen demand
- Ranolazine has minimal effect on:
a) Coronary perfusion
b) Heart rate and blood pressure
c) Intracellular sodium
d) Ventricular relaxation
Answer: b) Heart rate and blood pressure
- A common adverse effect is:
a) Constipation
b) Hypercalcemia
c) Severe bronchospasm
d) Mydriasis
Answer: a) Constipation
- Ranolazine may prolong the:
a) PR interval
b) QT interval
c) QRS duration only
d) ST segment only
Answer: b) QT interval
- Ranolazine is metabolized mainly by:
a) CYP3A4
b) MAO
c) Acetylcholinesterase
d) Xanthine oxidase
Answer: a) CYP3A4
- Compared with nitroglycerin, ranolazine causes:
a) Greater hypotension
b) Minimal blood pressure change
c) Severe reflex tachycardia
d) Strong vasodilation only
Answer: b) Minimal blood pressure change
- Ranolazine reduces intracellular calcium by improving function of the:
a) Sodium-calcium exchanger
b) Proton pump
c) Na⁺/K⁺ ATPase only
d) Calcium ATPase in bone
Answer: a) Sodium-calcium exchanger
FAQs
What is the mechanism of action of ranolazine?
Ranolazine inhibits the late sodium current in cardiac myocytes, reducing intracellular calcium overload.
How does ranolazine help in angina?
It improves myocardial relaxation and decreases oxygen demand during ischemia.
Does ranolazine significantly lower blood pressure?
No, it has minimal effects on blood pressure and heart rate.
Why can ranolazine prolong QT interval?
Because it affects cardiac repolarization currents.
What are common side effects of ranolazine?
Dizziness, constipation, headache, and nausea.
Why is ranolazine useful in patients intolerant to β blockers?
Because it controls angina without major hemodynamic effects.
References
Goodman & Gilman’s The Pharmacological Basis of Therapeutics – Antianginal Drugs
https://accessmedicine.mhmedical.com/book.aspx?bookid=3191
Katzung: Basic and Clinical Pharmacology – Drugs Used in Angina Pectoris
https://accessmedicine.mhmedical.com/content.aspx?bookid=3382
Tripathi: Essentials of Medical Pharmacology – Antianginal Drugs
https://www.jaypeedigital.com
Harrison’s Principles of Internal Medicine – Ischemic Heart Disease
https://accessmedicine.mhmedical.com

