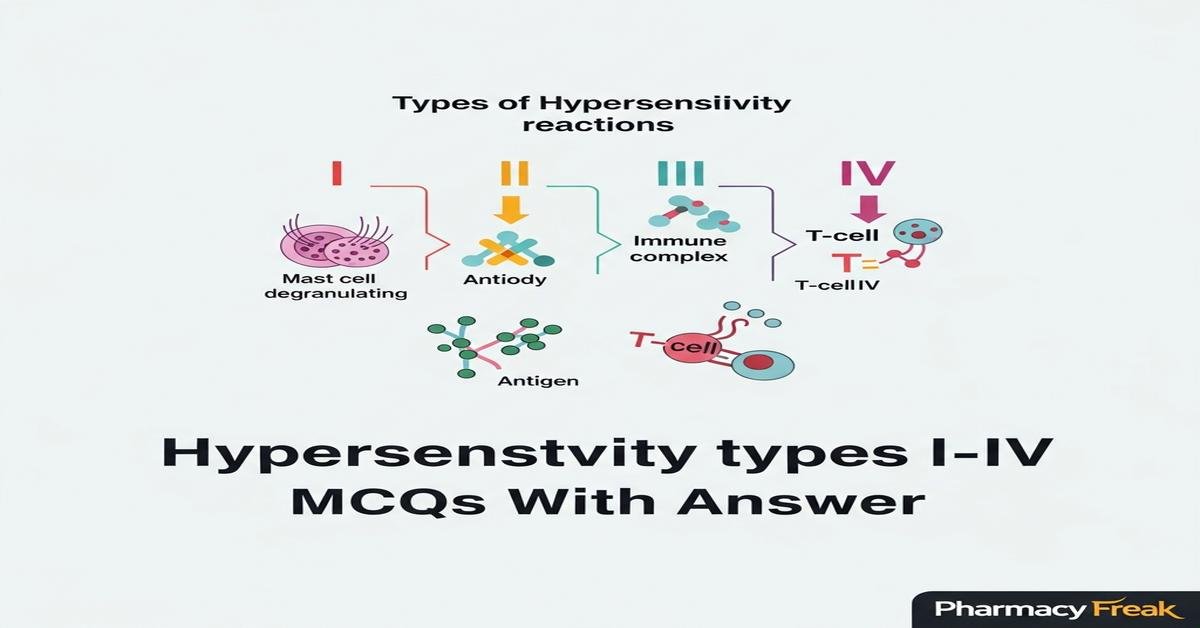
Introduction: This quiz collection on hypersensitivity types I–IV is designed for M.Pharm students preparing for advanced immunotechnology examinations. It concisely reviews mechanisms, key mediators, classic clinical examples, diagnostic tests and therapeutic approaches across immediate (Type I), antibody-mediated (Type II), immune-complex (Type III) and T-cell–mediated (Type IV) reactions. Questions emphasize mechanistic understanding, laboratory correlations such as Coombs, CH50 and specific IgE assays, and modern interventions including biologics and desensitization strategies. Use these MCQs to test applied knowledge, reinforce pathophysiology, and prepare for clinical and research contexts where precise distinctions among hypersensitivity types guide diagnosis and treatment decisions.
Q1. Which of the following best describes the primary mechanism underlying Type I hypersensitivity?
- Cross-linking of allergen-specific IgE on mast cells and basophils leading to degranulation
- Formation of immune complexes that deposit in vessel walls and activate complement
- Direct cytotoxicity by IgG and complement against target cells
- Delayed activation of macrophages by sensitized T lymphocytes
Correct Answer: Cross-linking of allergen-specific IgE on mast cells and basophils leading to degranulation
Q2. Which mediator is most responsible for prolonged bronchoconstriction in allergic asthma associated with Type I reactions?
- Histamine
- Prostaglandin D2
- Cysteinyl leukotrienes (LTC4, LTD4)
- Platelet-activating factor (PAF)
Correct Answer: Cysteinyl leukotrienes (LTC4, LTD4)
Q3. Which diagnostic approach is most appropriate to confirm IgE-mediated allergy to a specific inhalant antigen?
- Direct antiglobulin (Coombs) test
- Skin prick testing (wheal-and-flare) and serum-specific IgE assays (RAST/ImmunoCAP)
- CH50 complement hemolytic assay
- Delayed-type hypersensitivity patch testing
Correct Answer: Skin prick testing (wheal-and-flare) and serum-specific IgE assays (RAST/ImmunoCAP)
Q4. First-line emergency treatment for systemic anaphylaxis due to Type I hypersensitivity is:
- Intravenous antihistamine infusion
- Intramuscular epinephrine
- High-dose corticosteroids only
- Plasmapheresis
Correct Answer: Intramuscular epinephrine
Q5. Which of the following clinical conditions is a classic example of Type II hypersensitivity with receptor-modulating antibodies?
- Serum sickness
- Myasthenia gravis
- Contact dermatitis
- Allergic rhinitis
Correct Answer: Myasthenia gravis
Q6. The direct Coombs (direct antiglobulin) test is used to detect:
- Circulating immune complexes in serum
- Antibodies or complement components bound directly to the patient’s red blood cells
- Serum levels of specific IgE
- Functional integrity of the classical complement pathway
Correct Answer: Antibodies or complement components bound directly to the patient’s red blood cells
Q7. Which laboratory assay is commonly used to detect circulating immune complexes in suspected Type III hypersensitivity?
- Direct Coombs test
- C1q-binding assay for immune complexes
- Skin prick test
- Interferon-gamma release assay (IGRA)
Correct Answer: C1q-binding assay for immune complexes
Q8. What is the primary pathophysiological event in Type III hypersensitivity reactions?
- IgE-mediated mast cell degranulation
- Antibody-mediated complement lysis of host cells
- Deposition of antigen–antibody immune complexes in tissues with complement activation and neutrophil recruitment
- T-cell mediated macrophage activation causing granuloma formation
Correct Answer: Deposition of antigen–antibody immune complexes in tissues with complement activation and neutrophil recruitment
Q9. Which clinical syndrome is a prototypical systemic Type III hypersensitivity reaction?
- Immediate urticaria
- Serum sickness
- Goodpasture’s syndrome
- Type 1 diabetes mellitus
Correct Answer: Serum sickness
Q10. In severe immune complex–mediated vasculitis, which therapeutic intervention directly removes circulating pathogenic complexes?
- High-dose antihistamines
- Plasmapheresis (therapeutic plasma exchange)
- Topical corticosteroids
- Allergen-specific subcutaneous immunotherapy
Correct Answer: Plasmapheresis (therapeutic plasma exchange)
Q11. Type IV delayed-type hypersensitivity is primarily mediated by which immune mechanism?
- IgE cross-linking on basophils
- Activation of complement by IgM
- Th1 CD4+ T cells producing IFN-γ and activating macrophages
- Immune complex deposition and neutrophil activation
Correct Answer: Th1 CD4+ T cells producing IFN-γ and activating macrophages
Q12. The Mantoux (tuberculin) skin test exemplifies which hypersensitivity type?
- Type I immediate hypersensitivity
- Type II cytotoxic hypersensitivity
- Type III immune complex hypersensitivity
- Type IV delayed-type hypersensitivity
Correct Answer: Type IV delayed-type hypersensitivity
Q13. Contact dermatitis caused by poison ivy (urushiol) is predominantly mediated by which cell population?
- Mast cells and basophils
- B lymphocytes producing IgG
- Sensitized T lymphocytes (Th1 and cytotoxic T cells)
- Neutrophils recruited by immune complexes
Correct Answer: Sensitized T lymphocytes (Th1 and cytotoxic T cells)
Q14. Which laboratory test measures the functional integrity of the classical complement pathway?
- ELISA for specific IgE
- CH50 hemolytic assay
- Direct Coombs test
- Patch test for contact allergens
Correct Answer: CH50 hemolytic assay
Q15. Which drug class is most commonly associated with immediate IgE-mediated anaphylaxis due to hapten formation?
- Beta-lactam antibiotics (penicillins)
- Statins
- ACE inhibitors
- Proton pump inhibitors
Correct Answer: Beta-lactam antibiotics (penicillins)
Q16. What is the primary immunological mechanism by which allergen-specific desensitization (immunotherapy) reduces Type I reactions?
- Permanent deletion of allergen-specific B cells
- Induction of IgG “blocking” antibodies and regulatory T cells, reducing IgE-mediated activation
- Immediate neutralization of circulating IgE by epinephrine
- Increasing mast cell numbers to dilute response
Correct Answer: Induction of IgG “blocking” antibodies and regulatory T cells, reducing IgE-mediated activation
Q17. Which biologic drug is specifically designed to neutralize free IgE and is used in severe allergic asthma?
- Rituximab (anti-CD20)
- Infliximab (anti-TNFα)
- Omalizumab (anti-IgE monoclonal antibody)
- Abatacept (CTLA-4 Ig)
Correct Answer: Omalizumab (anti-IgE monoclonal antibody)
Q18. Antibody-dependent cell-mediated cytotoxicity (ADCC) in Type II reactions is primarily executed by which effector cells?
- Neutrophils via complement receptors
- Natural killer (NK) cells via FcγRIII (CD16)
- B cells via Fc receptors
- Platelets releasing mediators
Correct Answer: Natural killer (NK) cells via FcγRIII (CD16)
Q19. What is the typical time frame for clinical onset of serum sickness, a systemic Type III hypersensitivity?
- Within minutes of exposure
- 1–4 hours after exposure
- 7–14 days after antigen exposure
- Several months after exposure
Correct Answer: 7–14 days after antigen exposure
Q20. Which feature best distinguishes Type IV hypersensitivity from Types I–III?
- It is mediated by antibodies and complement
- It is immediate, occurring within seconds to minutes
- It is cell-mediated, often peaking 48–72 hours after antigen exposure
- It is driven by immune complex deposition in small vessels
Correct Answer: It is cell-mediated, often peaking 48–72 hours after antigen exposure

