
Table of Contents
Introduction
Thiazide diuretics are one of the most commonly prescribed classes of antihypertensive agents, especially in the U.S. They are highly effective in treating mild to moderate hypertension and are also useful in managing edema, calcium kidney stones, and heart failure.
Examples include:
- Hydrochlorothiazide (HCTZ)
- Chlorthalidone
- Indapamide
- Metolazone
Thiazides are recommended as first-line therapy for hypertension in JNC-8 and AHA/ACC guidelines, and frequently appear in USMLE, NCLEX, NAPLEX, and GPAT exams.
Stepwise Mechanism of Action of Thiazide Diuretics
- Site of Action – Distal Convoluted Tubule (DCT)
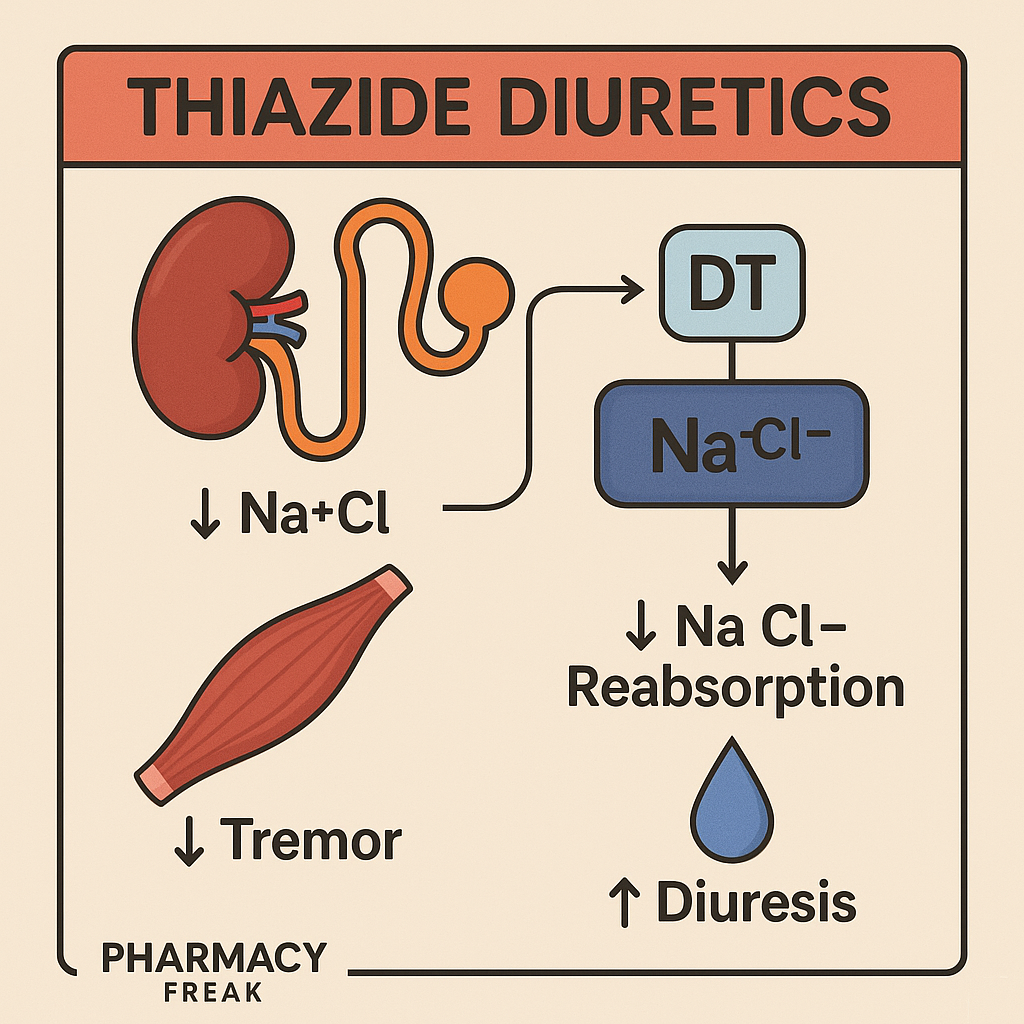
Thiazides act primarily at the early distal convoluted tubule in the nephron. - Inhibition of Na⁺/Cl⁻ Symporter
Thiazides block the Na⁺/Cl⁻ cotransporter (NCC) on the luminal membrane of DCT cells. This reduces sodium and chloride reabsorption. - Increased Sodium and Water Excretion
The net result is natriuresis and diuresis, which reduces plasma volume and cardiac output, lowering blood pressure. - Mild Vasodilation
Chronic use also leads to reduced peripheral vascular resistance, contributing to the long-term antihypertensive effect. - Calcium Reabsorption
Thiazides increase calcium reabsorption, making them beneficial in calcium-containing kidney stones and osteoporosis.
Pharmacokinetic Parameters of Thiazide Diuretics
| Parameter | General Values (varies by drug) |
|---|---|
| Bioavailability | 60–70% (oral) |
| Onset of Action | 1–2 hours (oral) |
| Half-life | HCTZ: ~6–15 hours; Chlorthalidone: ~40–60 hrs |
| Metabolism | Minimal; mostly excreted unchanged |
| Excretion | Renal |
Clinical Uses of Thiazide Diuretics
- Essential hypertension (first-line)
- Congestive heart failure (mild)
- Nephrolithiasis (calcium stones)
- Nephrogenic diabetes insipidus
- Edema due to liver cirrhosis or renal disease
- Osteoporosis (off-label)
Adverse Effects of Thiazide Diuretics
- Hypokalemia
- Hyponatremia
- Hypercalcemia
- Hyperuricemia → may precipitate gout
- Hyperglycemia
- Hyperlipidemia (mild increase in LDL, TG)
- Photosensitivity and rash
Contraindicated in sulfa-allergic patients and should be used with caution in diabetics and gout-prone individuals.
Comparative Analysis: Thiazide vs Loop Diuretics
| Feature | Thiazide Diuretics | Loop Diuretics (e.g., Furosemide) |
|---|---|---|
| Site of Action | Distal convoluted tubule | Thick ascending limb of loop of Henle |
| Sodium excretion | Moderate | High (potent diuresis) |
| Calcium effect | Retained (↑ reabsorption) | Lost (↑ excretion) |
| Use in CKD | Less effective at GFR <30 mL/min | Preferred in low GFR |
| Use in hypertension | First-line | Reserved for severe/resistant cases |
Practice MCQs
Q1. Thiazide diuretics act on which part of the nephron?
a. Proximal tubule
b. Loop of Henle
c. Distal convoluted tubule ✅
d. Collecting duct
Q2. The transporter inhibited by thiazides is:
a. Na⁺/K⁺/2Cl⁻ cotransporter
b. Na⁺/H⁺ exchanger
c. Na⁺/Cl⁻ symporter ✅
d. H⁺/K⁺ ATPase
Q3. Which electrolyte abnormality is commonly caused by thiazides?
a. Hyperkalemia
b. Hypokalemia ✅
c. Hypocalcemia
d. Hypermagnesemia
Q4. Which condition is uniquely improved by thiazide diuretics due to calcium retention?
a. Hypokalemia
b. Osteoporosis ✅
c. Hyperthyroidism
d. Asthma
Q5. Which of the following is NOT a typical adverse effect of thiazides?
a. Hyperglycemia
b. Hypocalcemia ✅
c. Hyperuricemia
d. Hyperlipidemia
Q6. Which of the following drugs has the longest half-life?
a. Hydrochlorothiazide
b. Chlorthalidone ✅
c. Metolazone
d. Indapamide
Q7. In a patient with gout, thiazides should be:
a. Used freely
b. Avoided or used cautiously ✅
c. Combined with allopurinol
d. Preferred over loop diuretics
Q8. What is a unique benefit of thiazides in nephrolithiasis?
a. Reduces sodium
b. Reduces uric acid
c. Increases calcium excretion
d. Reduces calcium excretion ✅
Q9. Which of the following metabolic effects is NOT associated with thiazide use?
a. Hyperglycemia
b. Hypernatremia ✅
c. Hyperuricemia
d. Hyperlipidemia
Q10. Thiazides are contraindicated in:
a. Gout
b. Heart failure
c. Sulfa allergy ✅
d. Pregnancy
FAQs
Q1: Can thiazides be used in chronic kidney disease (CKD)?
They are less effective when GFR <30 mL/min. Loop diuretics are preferred in advanced CKD.
Q2: Are thiazides potassium-sparing?
No. They cause potassium loss and are often paired with potassium-sparing agents.
Q3: Do thiazides cause calcium retention?
Yes, which is helpful in nephrolithiasis and osteoporosis.
Q4: How soon do thiazides start lowering blood pressure?
They begin to work within 2 hours, with full effect in 2–4 weeks.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- American College of Cardiology (ACC) Guidelines
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK482179/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com