
Table of Contents
Introduction
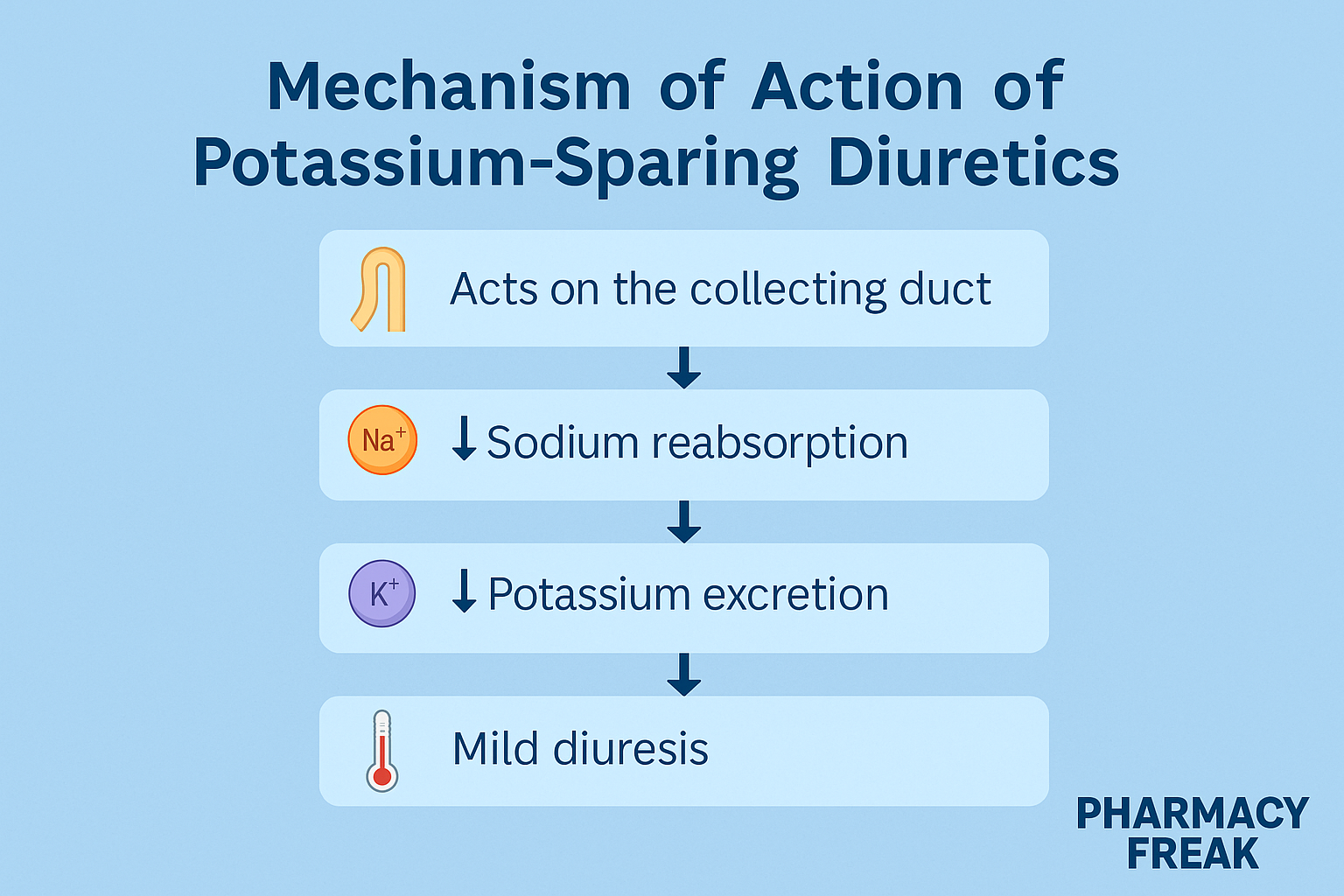
Potassium-sparing diuretics are a unique subclass of diuretics that help conserve potassium levels while promoting mild diuresis. Unlike other diuretics, they do not cause hypokalemia, making them ideal as adjunct therapy with thiazide or loop diuretics.
These drugs are grouped into two types:
- Aldosterone antagonists:
- Spironolactone
- Eplerenone
- Epithelial sodium channel (ENaC) blockers:
- Amiloride
- Triamterene
These drugs are tested frequently in USMLE, NCLEX, GPAT, NAPLEX, and used in treating heart failure, hypertension, hyperaldosteronism, and hypokalemia.
Stepwise Mechanism of Action of Potassium-Sparing Diuretics
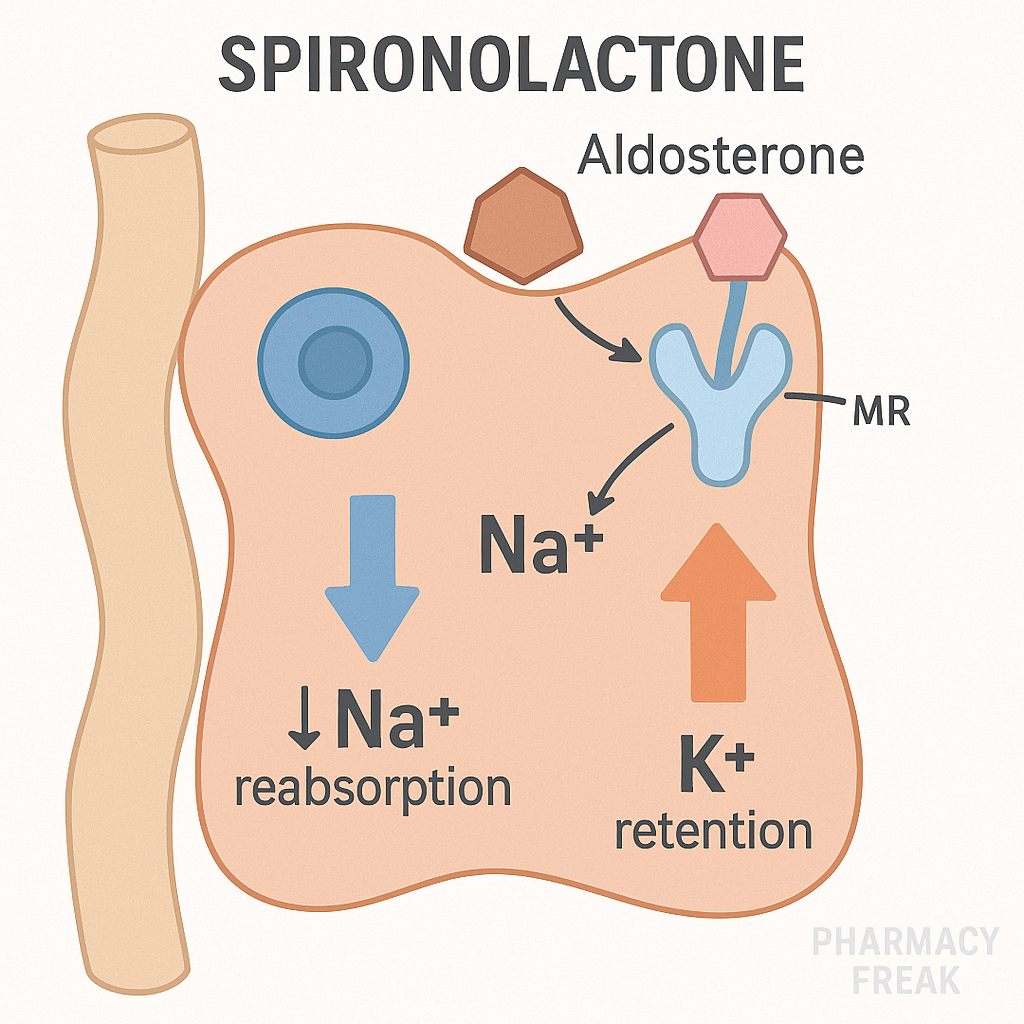
Aldosterone Antagonists (e.g., Spironolactone)
- Site of action – Collecting duct (principal cells)
Spironolactone and eplerenone act on intracellular mineralocorticoid receptors in the distal nephron. - Blockade of aldosterone effects
They prevent aldosterone-mediated expression of ENaC and Na⁺/K⁺ ATPase, reducing sodium reabsorption and potassium excretion. - Net result
- Mild natriuresis
- Potassium retention
- Reduction in blood pressure
- Decreased fibrosis and remodeling in heart failure

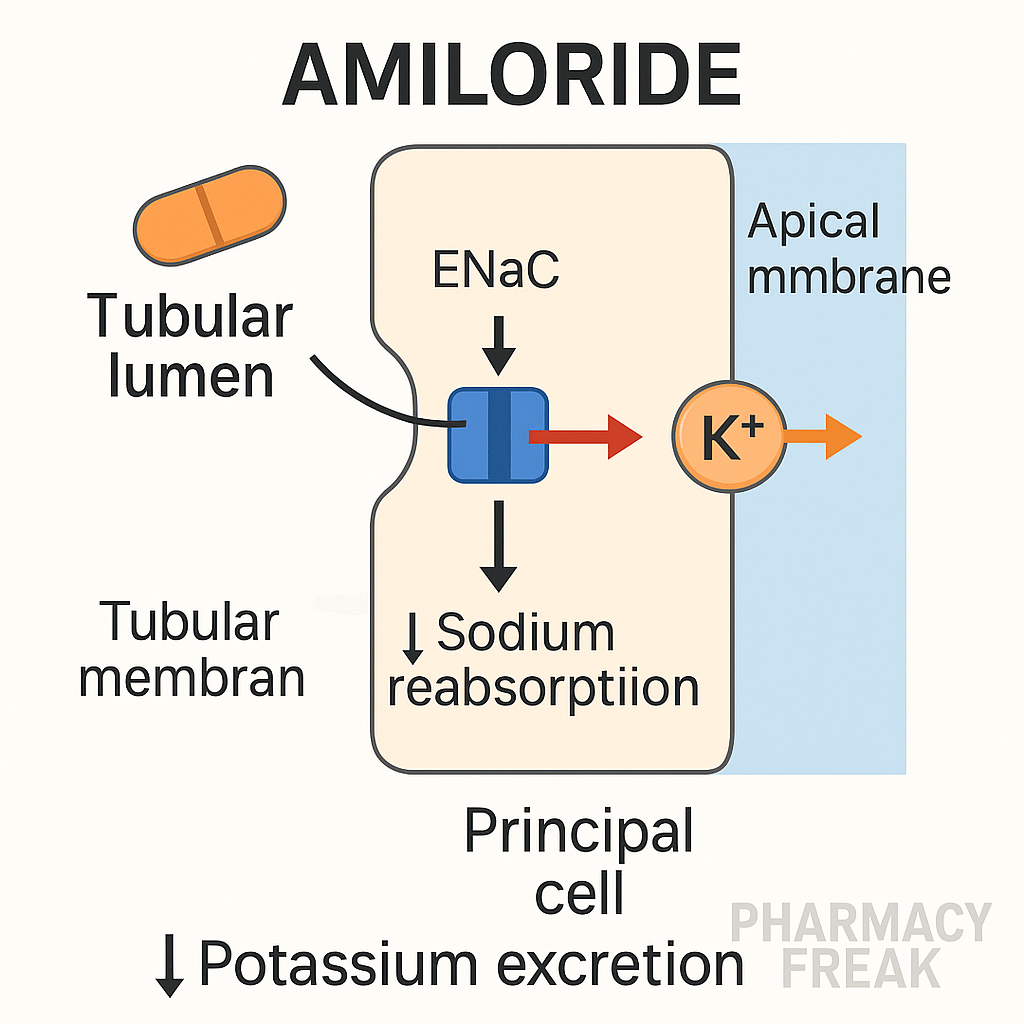
ENaC Blockers (e.g., Amiloride, Triamterene)
- Direct blockade of epithelial sodium channels
These drugs inhibit ENaC channels in the luminal membrane of principal cells, reducing sodium reabsorption directly. - Conservation of potassium
Sodium-potassium exchange is reduced → less potassium is secreted → prevention of hypokalemia.
Pharmacokinetic Parameters of Potassium-Sparing Diuretics
| Drug | Absorption (Oral) | Half-life | Metabolism | Excretion |
|---|---|---|---|---|
| Spironolactone | 60–90% | 1.4 hours (active metabolite: 18–23 hrs) | Hepatic | Renal/Bile |
| Eplerenone | ~70% | 4–6 hours | CYP3A4 | Renal/Fecal |
| Amiloride | ~15–25% | 6–9 hours | Minimal | Renal |
| Triamterene | ~30–70% | 4–6 hours | Hepatic | Renal |
Clinical Uses of Potassium-Sparing Diuretics
- Heart failure (esp. Spironolactone in HFrEF)
- Resistant hypertension
- Primary hyperaldosteronism
- Edema associated with liver cirrhosis
- Hypokalemia induced by thiazides/loops
- Polycystic ovarian syndrome (PCOS) – off-label use of spironolactone
- Liddle syndrome – amiloride is the drug of choice
Adverse Effects of Potassium-Sparing Diuretics
- Hyperkalemia – major and potentially life-threatening
- Gynecomastia, impotence, menstrual irregularities (esp. spironolactone due to antiandrogen effects)
- GI upset, nausea
- Metabolic acidosis (rare)
- Kidney stones (with triamterene)
Comparative Analysis: Spironolactone vs Amiloride
| Feature | Spironolactone | Amiloride |
|---|---|---|
| Mechanism | Aldosterone receptor antagonist | ENaC blocker |
| Onset of action | Delayed | Rapid |
| Androgen effects | Yes (antiandrogenic) | No |
| Hyperkalemia risk | High | Moderate |
| Use in PCOS | Yes | No |
| Use in Liddle syndrome | No | Yes |
Practice MCQs
Q1. Potassium-sparing diuretics act on which part of the nephron?
a. Proximal tubule
b. Loop of Henle
c. Distal convoluted tubule
d. Collecting duct ✅
Q2. Which of the following is a direct ENaC blocker?
a. Spironolactone
b. Eplerenone
c. Amiloride ✅
d. Furosemide
Q3. What is the major risk associated with potassium-sparing diuretics?
a. Hypokalemia
b. Hyperkalemia ✅
c. Hypocalcemia
d. Dehydration
Q4. Which potassium-sparing diuretic has antiandrogenic effects?
a. Amiloride
b. Spironolactone ✅
c. Triamterene
d. Eplerenone
Q5. Which condition is best treated with amiloride?
a. PCOS
b. Diabetes insipidus
c. Liddle syndrome ✅
d. Cushing’s disease
Q6. What is the mechanism of action of spironolactone?
a. ENaC inhibition
b. Na⁺/Cl⁻ cotransporter inhibition
c. Mineralocorticoid receptor antagonism ✅
d. Na⁺/K⁺/2Cl⁻ symporter inhibition
Q7. Eplerenone differs from spironolactone in that it:
a. Has shorter half-life
b. Does not cause hyperkalemia
c. Has fewer endocrine side effects ✅
d. Is more potent diuretic
Q8. Hyperkalemia with potassium-sparing diuretics is more likely when combined with:
a. NSAIDs ✅
b. Beta-blockers
c. Calcium channel blockers
d. Thiazides
Q9. Triamterene causes which rare side effect?
a. Kidney stones ✅
b. Gynecomastia
c. Hypokalemia
d. Hypercalcemia
Q10. Which is a potassium-sparing diuretic and aldosterone antagonist?
a. Amiloride
b. Spironolactone ✅
c. Hydrochlorothiazide
d. Furosemide
FAQs
Q1: Can potassium-sparing diuretics be used alone?
Yes, but due to weak diuretic effect, they’re mainly used with thiazides or loops to prevent potassium loss.
Q2: Which one is preferred in heart failure?
Spironolactone, as it improves survival in HFrEF patients (RALES trial).
Q3: What labs should be monitored during therapy?
Serum potassium and creatinine, to avoid hyperkalemia and nephrotoxicity.
Q4: Are they safe in pregnancy?
Not routinely recommended; spironolactone has antiandrogenic effects and should be avoided.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- AHA Guidelines for Hypertension
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK470437/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com