
Table of Contents
Introduction
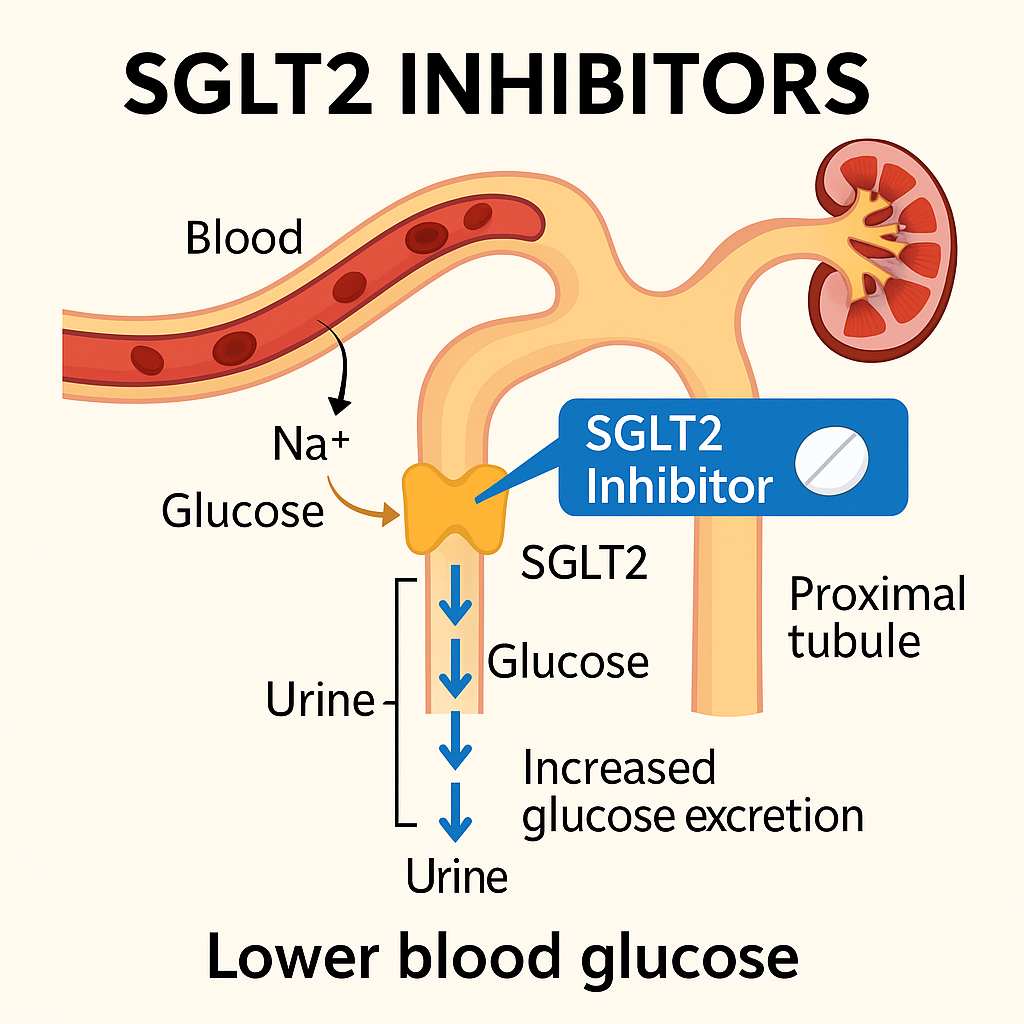
SGLT2 Inhibitors, or sodium-glucose co-transporter 2 inhibitors, are a newer class of oral antidiabetic drugs that reduce blood glucose levels by promoting urinary glucose excretion. Unlike insulin-dependent drugs, they work via the kidneys and help in both glycemic control and weight reduction.
Commonly used SGLT2 inhibitors include:
- Canagliflozin
- Dapagliflozin
- Empagliflozin
- Ertugliflozin
These drugs are now also used for cardiovascular protection and chronic kidney disease, in addition to type 2 diabetes management. Highly relevant for USMLE, NCLEX, GPAT, and NEET-PG prep.
Stepwise Mechanism of Action of SGLT2 Inhibitors
- Target site – Proximal convoluted tubule
SGLT2 inhibitors act on the proximal renal tubules, where SGLT2 transporters reabsorb 90% of filtered glucose. - Inhibition of SGLT2 transporter
These drugs selectively inhibit SGLT2, reducing glucose reabsorption from the renal tubule back into the bloodstream. - Increased urinary glucose excretion (UGE)
Glucose is excreted in urine, leading to reduced plasma glucose levels and caloric loss. - Reduction in fasting and postprandial glucose
Glycemic control improves independent of insulin, reducing risk of hypoglycemia. - Additional systemic benefits
They also lead to weight loss, mild diuresis, reduced blood pressure, and cardioprotective and nephroprotective effects.
Pharmacokinetic Parameters of SGLT2 Inhibitors
| Drug | Bioavailability | Half-life | Metabolism | Excretion |
|---|---|---|---|---|
| Canagliflozin | ~65% | 10–13 hrs | Hepatic (UGT1A9/UGT2B4) | Renal (~33%) |
| Dapagliflozin | ~78% | 12–13 hrs | Hepatic (UGT1A9) | Renal (~75%) |
| Empagliflozin | ~78% | 12 hrs | Minimal hepatic metabolism | Renal (~55%) |
Clinical Uses of SGLT2 Inhibitors
- Type 2 diabetes mellitus
- Heart failure with reduced or preserved ejection fraction (HFrEF, HFpEF)
- Chronic kidney disease (CKD)
- Weight management (indirect benefit)
- Reduction in cardiovascular risk (e.g., empagliflozin in EMPA-REG OUTCOME trial)
Adverse Effects of SGLT2 Inhibitors
- Genital and urinary tract infections (common due to glucosuria)
- Volume depletion, hypotension
- Diabetic ketoacidosis (euglycemic DKA – rare but serious)
- Increased urination (polyuria)
- Fournier’s gangrene (very rare)
- Fracture risk and amputation (canagliflozin – earlier warning, now revised)
Comparative Analysis: SGLT2 Inhibitors vs Other Oral Antidiabetics
| Feature | SGLT2 Inhibitors | Other Oral Drugs |
|---|---|---|
| Hypoglycemia risk | Very low | Moderate to high (sulfonylureas) |
| Weight impact | Weight loss | Neutral or weight gain |
| Insulin dependence | Independent | Mostly dependent |
| Cardiovascular benefit | Yes (empagliflozin, dapagliflozin) | Not consistent |
| Route of excretion | Renal | Mostly hepatic or mixed |
Practice MCQs
Q1. SGLT2 inhibitors reduce blood glucose primarily by:
a. Enhancing insulin sensitivity
b. Blocking glucose absorption in the intestine
c. Inhibiting renal glucose reabsorption ✅
d. Stimulating insulin secretion
Q2. Which transporter is blocked by SGLT2 inhibitors?
a. SGLT1
b. SGLT2 ✅
c. GLUT4
d. Na⁺/K⁺ pump
Q3. Where is the SGLT2 transporter located?
a. Loop of Henle
b. Distal tubule
c. Proximal convoluted tubule ✅
d. Collecting duct
Q4. Which of the following is NOT a known benefit of SGLT2 inhibitors?
a. Weight loss
b. Increased insulin production ✅
c. Cardiovascular protection
d. Lower blood pressure
Q5. What serious but rare complication can occur with SGLT2 inhibitors?
a. Diabetic retinopathy
b. Euglycemic ketoacidosis ✅
c. Thyroid cancer
d. Hypercalcemia
Q6. Which drug has the strongest evidence for cardiovascular benefit?
a. Sitagliptin
b. Glibenclamide
c. Empagliflozin ✅
d. Acarbose
Q7. The increased urination from SGLT2 inhibitors is due to:
a. Osmotic diuresis from glucose ✅
b. Water channel blockage
c. Increased ADH
d. Loop of Henle inhibition
Q8. The EMPA-REG OUTCOME trial showed that empagliflozin:
a. Raises LDL
b. Increases fracture risk
c. Reduces cardiovascular mortality ✅
d. Stimulates insulin release
Q9. Which patient population needs caution with SGLT2 inhibitors?
a. Obese individuals
b. Patients with low GFR ✅
c. Type 2 diabetics with good renal function
d. Non-diabetic hypertensives
Q10. Which of the following is a common side effect of SGLT2 inhibitors?
a. Hypoglycemia
b. Genital infections ✅
c. Hyperkalemia
d. Hepatitis
FAQs
Q1: Can SGLT2 inhibitors be used in type 1 diabetes?
Not routinely. Risk of euglycemic ketoacidosis makes them unsuitable unless under special protocols.
Q2: Do SGLT2 inhibitors cause hypoglycemia?
No, unless combined with insulin or sulfonylureas.
Q3: Are they safe in kidney disease?
Yes, especially dapagliflozin and empagliflozin, which are FDA-approved for CKD.
Q4: Should SGLT2 inhibitors be taken with food?
They can be taken with or without food, usually once daily in the morning.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- ADA Guidelines
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK513321/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com