
Table of Contents
Introduction
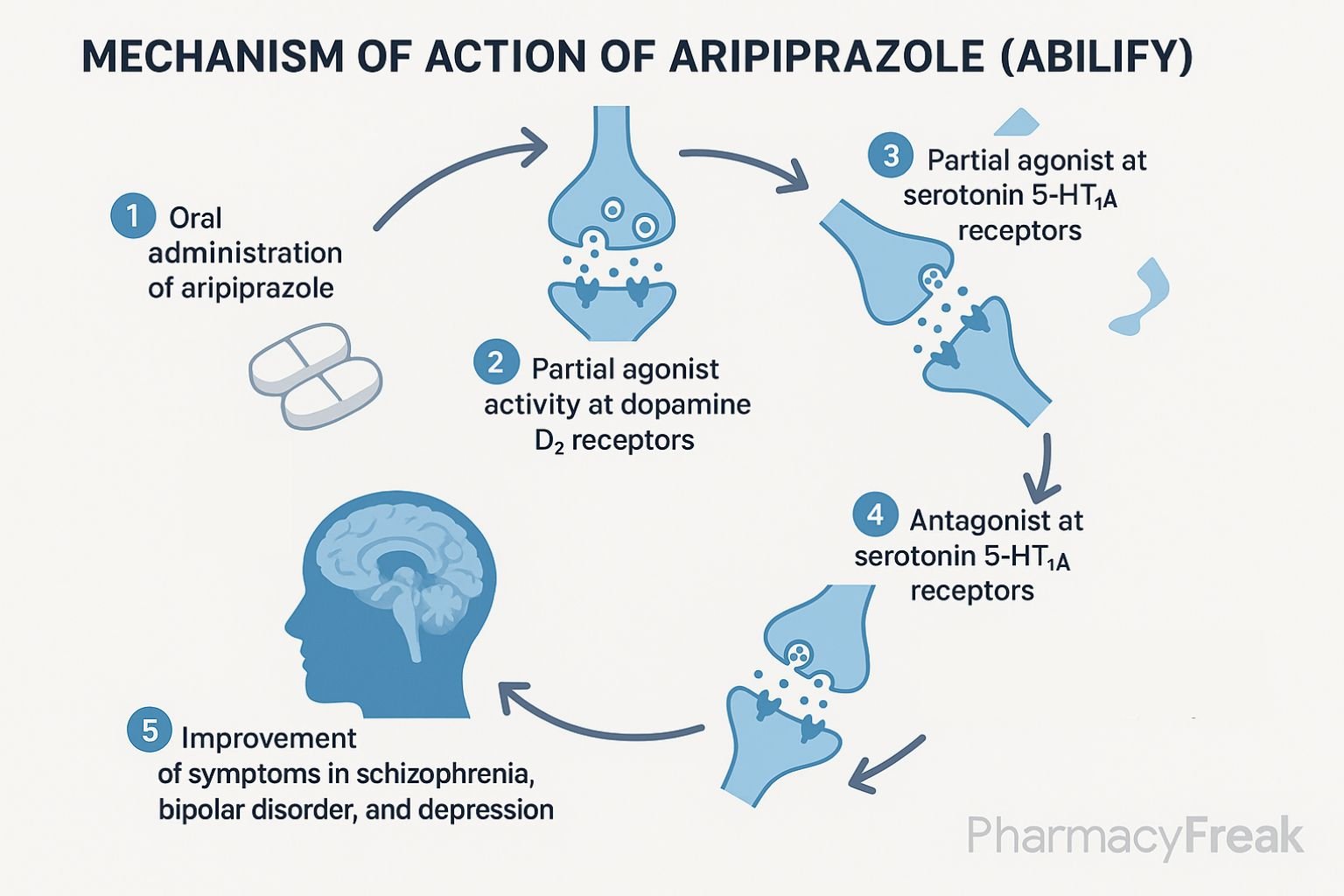
Aripiprazole is an atypical antipsychotic used to treat schizophrenia, bipolar disorder, major depressive disorder (as adjunct), irritability in autism, and Tourette’s syndrome. Its unique action as a dopamine D₂ partial agonist, along with effects on serotonin receptors, sets it apart from other agents, providing antipsychotic efficacy with a lower risk of certain side effects.

Step-by-Step Mechanism of Action
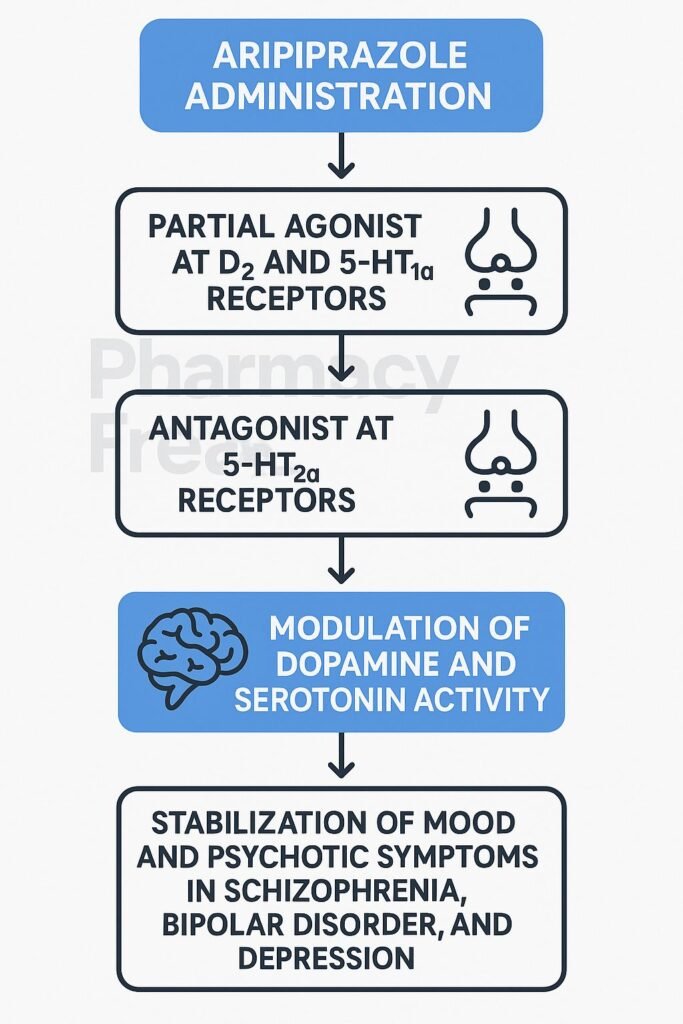
- Partial agonism at dopamine D₂ receptors
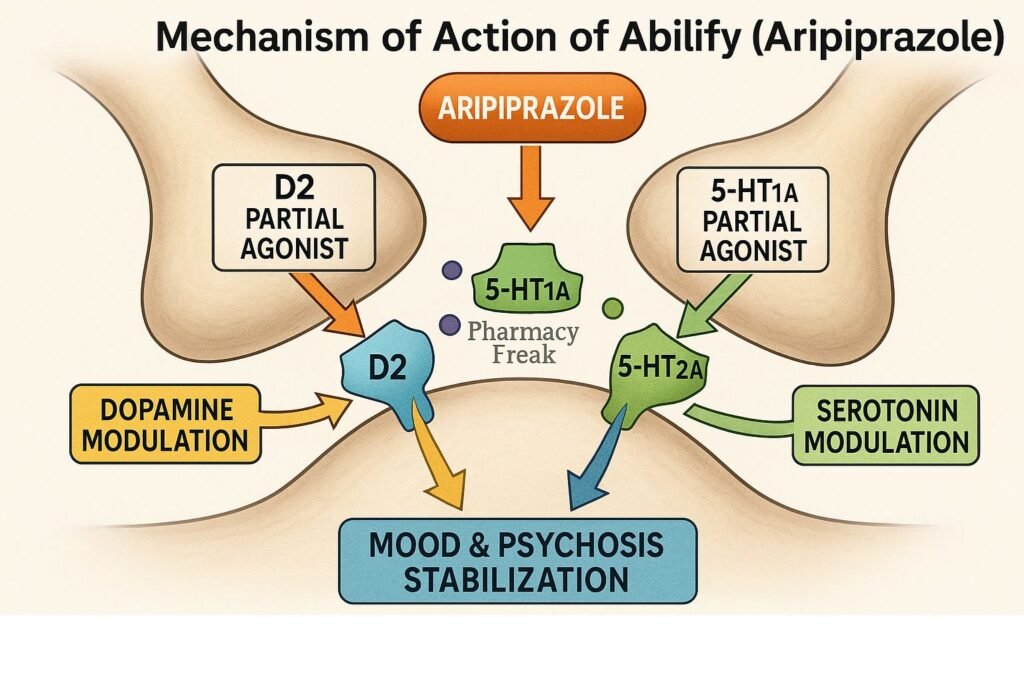
Acts as a dopamine D₂ receptor partial agonist—modulating dopamine activity by inhibiting excess signaling while providing baseline activation to avoid severe dopamine blockade. - Partial agonism at serotonin 5-HT₁A receptors
Enhances mood and anxiety regulation via 5-HT₁A receptor activation. - Antagonism at serotonin 5-HT₂A receptors
Reduces dopaminergic overstimulation and mitigates extrapyramidal symptoms (EPS). - Additional receptor effects
- Partial agonist at D₃ receptors
- Antagonist at 5-HT₂C and 5-HT₇ receptors
- Minimal affinity for histaminergic, muscarinic, and adrenergic receptors—resulting in less sedation, weight gain, and metabolic side effects.
- Neurotransmission modulation
Combined receptor actions regulate dopamine and serotonin pathways, improving psychosis, mood, and cognition with reduced adverse profiles.

Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route | Oral tablet, or long-acting injectable (IM) |
| Bioavailability | ~87% |
| Time to Peak (Tmax) | 3–5 hours |
| Protein Binding | ~99% |
| Metabolism | Hepatic via CYP3A4 and CYP2D6 |
| Half-life | 75 hours (oral); 30–46 days (LAI) |
| Excretion | Urine (25%), feces (60%) |
Clinical Uses
- Schizophrenia
- Acute and maintenance bipolar mania or mixed episodes
- Adjunctive therapy in major depressive disorder
- Irritability in autism
- Tourette’s syndrome
Adverse Effects
- Akathisia (most common)
- Nausea, vomiting, constipation
- Headache and insomnia
- Low risk of weight gain, sedation, metabolic syndrome
- Rare: orthostatic hypotension
- Lower risk for EPS compared to typical antipsychotics
Comparative Analysis
| Agent | D₂ Receptor Action | 5‑HT₂A Antagonism | EPS Risk | Metabolic Risk |
|---|---|---|---|---|
| Aripiprazole | Partial agonist | Yes | Low | Low |
| Risperidone | Antagonist | Yes | Moderate | Moderate |
| Olanzapine | Antagonist | Yes | Low | High |
MCQs
- Aripiprazole acts at D₂ receptors as a:
a) Full antagonist b) Full agonist c) Partial agonist d) Inverse agonist
Answer: c) Partial agonist - Its effect on 5-HT₁A receptors is:
a) Antagonist b) Partial agonist c) Full agonist d) No action
Answer: b) Partial agonist - Aripiprazole’s interaction at 5-HT₂A receptors is:
a) Agonist b) Partial agonist c) Antagonist d) Inverse agonist
Answer: c) Antagonist - Compared to olanzapine, metabolic risk is:
a) Higher b) Similar c) Lower d) Unstudied
Answer: c) Lower - Akathisia during treatment is:
a) Uncommon b) Common c) Never occurs d) Extremely rare
Answer: b) Common - Long-acting injectable half-life is:
a) 1 day b) 75 hours c) 30–46 days d) 1 year
Answer: c) 30–46 days - Which enzyme primarily metabolizes aripiprazole?
a) CYP3A4 b) CYP2D6 c) Both CYP3A4 and CYP2D6 d) CYP1A2
Answer: c) Both CYP3A4 and CYP2D6 - It has the lowest risk for:
a) EPS b) Weight gain c) Akathisia d) Orthostatic hypotension
Answer: b) Weight gain - Aripiprazole’s protein binding is approximately:
a) 50% b) 75% c) 99% d) 100%
Answer: c) 99% - Aripiprazole is NOT indicated for:
a) Autism irritability b) Major depressive disorder adjunct c) Tourette’s syndrome d) Dementia-related psychosis
Answer: d) Dementia-related psychosis
FAQs
1. Does aripiprazole cause weight gain?
It has a low metabolic risk, with minimal weight gain compared to other antipsychotics.
2. Can it be used for depression?
Yes, as an adjunct in treatment-resistant major depressive disorder.
3. What is the risk of akathisia?
Akathisia is common and may require dose adjustment or symptomatic treatment.
4. Is a long-acting injectable available?
Yes, the long-acting IM formulation can be administered monthly or quarterly.
5. Are dose adjustments needed in liver impairment?
Yes—lower initial doses are recommended for moderate hepatic impairment.
References
- FDA Label: Aripiprazole (Abilify)
- DrugBank: Aripiprazole Summary
- StatPearls: Aripiprazole Pharmacology
- PubMed Review: Multimodal Mechanism of Aripiprazole
- PMC: Partial agonist mechanism and clinical outcomes


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com