
Helminthic infections are a major public health problem in tropical and developing countries. They are caused by parasitic worms such as roundworms, tapeworms, and flukes. Anthelmintic drugs are used to eliminate these parasites from the body either by killing them or by expelling them through the intestine. These drugs differ in their mechanism of action and spectrum of activity depending on the type of worm.
This blog from Pharmacy Freak explains the classification, uses, drug of choice, side effects, and updated treatment guidelines for anthelmintic therapy.
Table of Contents
What is Anthelmintic Drug
Anthelmintic drugs are pharmacological agents used to treat infections caused by parasitic helminths. These include roundworms (nematodes), flatworms (cestodes and trematodes), and tissue-invading larvae.
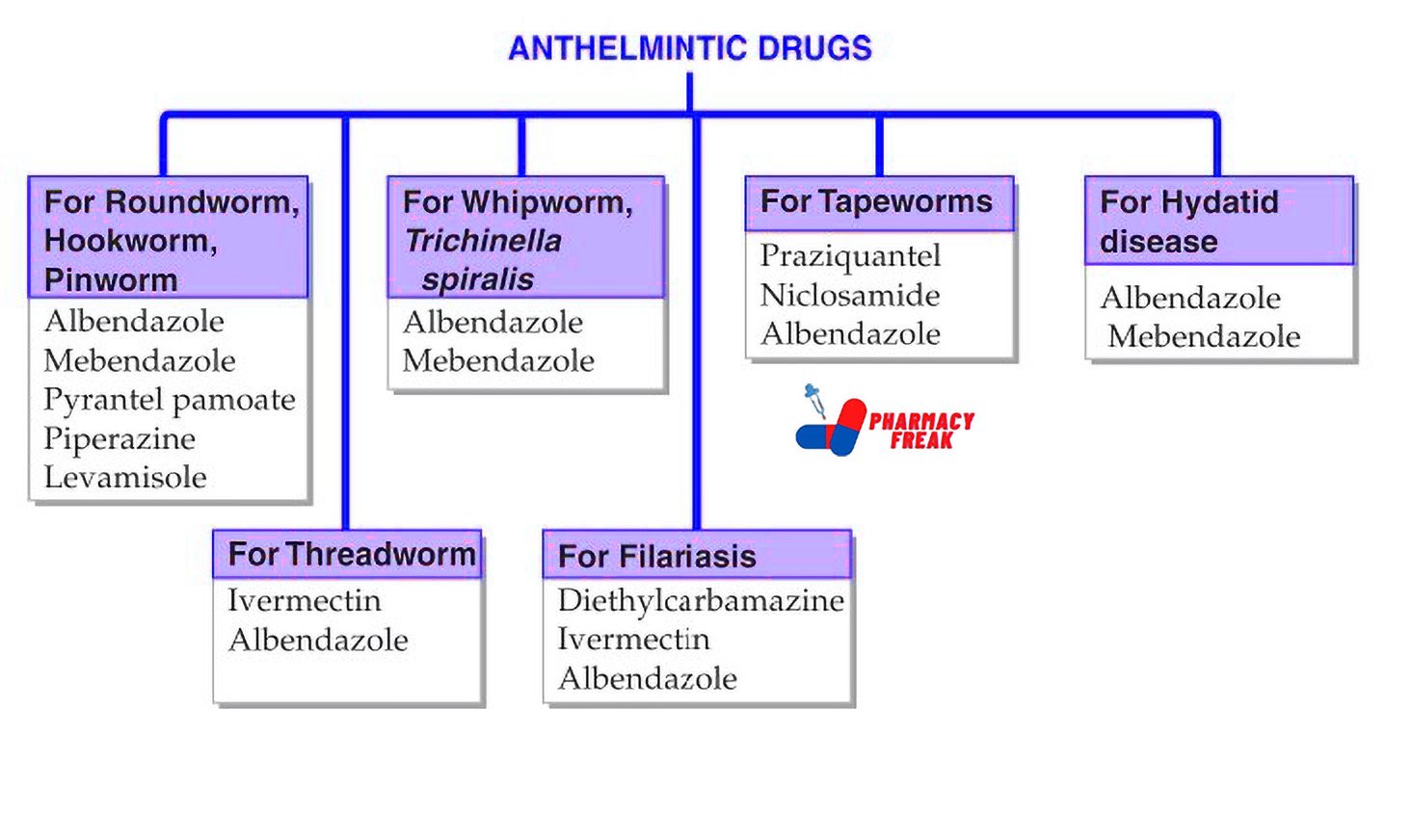
Classification of Anthelmintic Drug (KD Tripathi)
- For Roundworm, Hookworm, Pinworm: Albendazole, Mebendazole, Pyrantel pamoate, Piperazine, Levamisole
- For Whipworm, Trichinella spiralis: Albendazole, Mebendazole
- For Threadworm: Ivermectin, Albendazole
- For Filariasis: Diethylcarbamazine, Ivermectin, Albendazole
- For Tapeworms: Praziquantel, Niclosamide, Albendazole
- For Hydatid disease: Albendazole, Mebendazole
Classification of Anthelmintic Drug (General)
Anthelmintic drugs are classified based on the type of helminth they are effective against
- Drugs acting against Nematodes (Roundworms)
Albendazole
Mebendazole
Pyrantel pamoate
Levamisole
Piperazine
Ivermectin
Diethylcarbamazine (DEC) - Drugs acting against Cestodes (Tapeworms)
Praziquantel
Albendazole
Niclosamide - Drugs acting against Trematodes (Flukes)
Praziquantel
Triclabendazole
Metrifonate
Bithionol
Oxamniquine - Broad-Spectrum Anthelmintics
Albendazole
Mebendazole
Ivermectin
Praziquantel
Uses
- Roundworm (Ascaris lumbricoides) – Albendazole or Mebendazole
- Hookworm (Ancylostoma, Necator) – Albendazole
- Threadworm (Strongyloides stercoralis) – Ivermectin
- Whipworm (Trichuris trichiura) – Mebendazole
- Pinworm (Enterobius vermicularis) – Mebendazole or Pyrantel pamoate
- Filariasis (Wuchereria bancrofti) – Diethylcarbamazine
- Onchocerciasis – Ivermectin
- Hydatid cyst (Echinococcus granulosus) – Albendazole
- Cysticercosis (Taenia solium larval stage) – Albendazole + Steroid
- Taeniasis (Taenia saginata, Taenia solium) – Praziquantel or Niclosamide
- Schistosomiasis – Praziquantel
- Liver fluke (Fasciola hepatica) – Triclabendazole
Drug of Choice Highlights
- Ascariasis – Albendazole single dose
- Hookworm infection – Albendazole or Mebendazole
- Enterobiasis – Albendazole or Pyrantel with repetition after 2 weeks
- Strongyloidiasis – Ivermectin for systemic infections
- Filariasis – Diethylcarbamazine for 12 days
- Onchocerciasis – Ivermectin every 6 months
- Hydatid disease – Albendazole for pre- and post-surgical use
- Neurocysticercosis – Albendazole + corticosteroids + antiepileptics
- Schistosomiasis – Praziquantel single dose
- Fascioliasis – Triclabendazole
Side Effects
- Albendazole – Abdominal pain, dizziness, headache, reversible liver enzyme elevation
- Mebendazole – GI upset, hypersensitivity, neutropenia with prolonged use
- Pyrantel pamoate – Nausea, cramps, headache, neuromuscular blockade in high doses
- Levamisole – Nausea, vomiting, leukopenia, agranulocytosis
- Piperazine – Dizziness, neurotoxicity, contraindicated in epileptics
- Ivermectin – Pruritus, rash, lymphadenitis, Mazotti reaction in onchocerciasis
- Diethylcarbamazine – Fever, headache, myalgia, allergic reaction to dying microfilariae
- Praziquantel – Drowsiness, abdominal discomfort, increased liver enzymes
- Triclabendazole – GI symptoms, elevated liver enzymes
- Niclosamide – GI irritation, mild nausea
Updated Clinical Pearls
- Albendazole is preferred over mebendazole due to better efficacy and broader spectrum
- Ivermectin is highly effective against both intestinal and tissue nematodes like Strongyloides and Onchocerca
- Diethylcarbamazine is the drug of choice for bancroftian and brugian filariasis but contraindicated in onchocerciasis
- Praziquantel is effective against both cestodes and trematodes, making it useful for multiple parasitic infections
- Steroids are co-administered in neurocysticercosis to reduce inflammation caused by dying larvae
- Single-dose albendazole mass deworming is a WHO-recommended strategy in endemic regions
- Repeated treatment may be necessary in pinworm infection due to reinfection from contaminated surroundings
References
- Tripathi KD. Essentials of Medical Pharmacology. 7th ed. New Delhi: Jaypee Brothers Medical Publishers; 2013. p. 902–907
- Gupta S, Garg A. Review of Pharmacology. 15th ed. New Delhi: Jaypee Brothers Medical Publishers; 2023. p. 308–309
- Brunton LL, Chabner BA, Knollmann BC, editors. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill Education; 2011. p. 1589–1595
Related Links


I am a Registered Pharmacist under the Pharmacy Act, 1948, and the founder of PharmacyFreak.com. I hold a Bachelor of Pharmacy degree from Rungta College of Pharmaceutical Science and Research. With a strong academic foundation and practical knowledge, I am committed to providing accurate, easy-to-understand content to support pharmacy students and professionals. My aim is to make complex pharmaceutical concepts accessible and useful for real-world application.
Mail- Sachin@pharmacyfreak.com