
Table of Contents
Introduction
Thiazolidinediones (TZDs), also known as glitazones, are oral antidiabetic drugs used to improve insulin sensitivity in patients with type 2 diabetes mellitus. Unlike insulin secretagogues, TZDs do not stimulate insulin release—they enhance the body’s response to insulin.
Common examples include:
- Pioglitazone
- Rosiglitazone
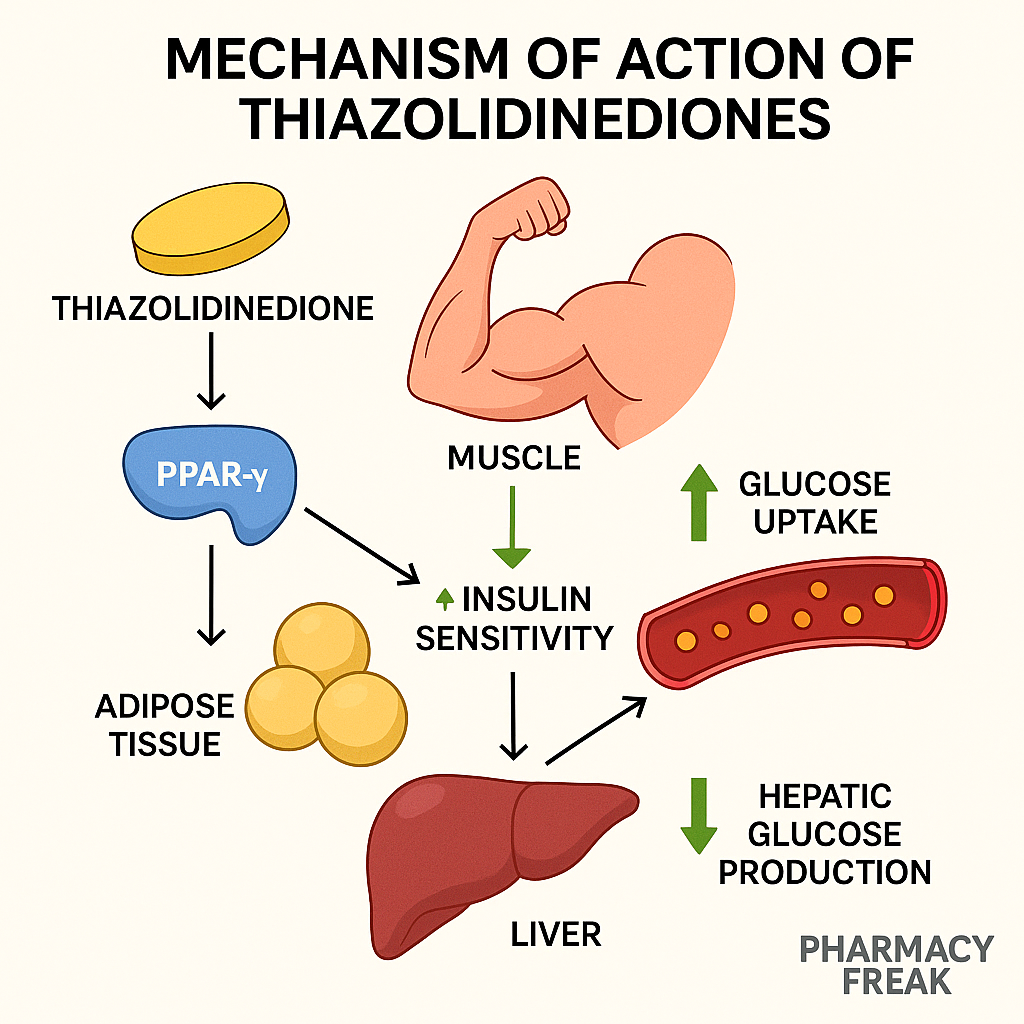
They act by binding to PPAR-γ (peroxisome proliferator-activated receptor gamma) and modulating gene transcription, leading to improved glucose uptake in peripheral tissues. TZDs are frequently asked about in USMLE, GPAT, NCLEX, and NIPER pharmacology modules.
Stepwise Mechanism of Action of Thiazolidinediones
- Binding to PPAR-γ
TZDs bind to PPAR-γ, a nuclear receptor primarily found in adipose tissue, muscle, and liver. - PPAR-γ activation and gene modulation
Activated PPAR-γ forms a heterodimer with retinoid X receptor (RXR), regulating the transcription of insulin-responsive genes. - Enhanced insulin sensitivity
Gene activation increases GLUT4 expression, adiponectin, and other insulin-sensitizing proteins in skeletal muscle and adipose tissue. - Reduced hepatic glucose production
In the liver, TZDs reduce gluconeogenesis, contributing to lower fasting blood glucose levels. - Redistribution of fat
TZDs promote subcutaneous fat storage over visceral fat accumulation, reducing insulin resistance. - No stimulation of insulin release
Unlike sulfonylureas or glinides, TZDs do not induce hypoglycemia when used alone.
Pharmacokinetic Parameters of TZDs
| Drug | Absorption | Half-life | Metabolism | Excretion |
|---|---|---|---|---|
| Pioglitazone | ~80% | 3–7 hrs (active metabolite: 16–24 hrs) | Hepatic (CYP2C8) | Fecal and renal |
| Rosiglitazone | ~99% | ~3–4 hrs | Hepatic (CYP2C8, CYP2C9) | Renal/Fecal |
Clinical Uses of TZDs
- Type 2 diabetes mellitus (monotherapy or with metformin, sulfonylureas, or insulin)
- Insulin resistance syndromes
- Polycystic ovarian syndrome (PCOS) – off-label use
- Non-alcoholic fatty liver disease (NAFLD) – under research
Adverse Effects of TZDs
- Weight gain (due to fluid retention and adipose accumulation)
- Edema and fluid retention → may exacerbate heart failure
- Increased risk of fractures (especially in women)
- Anemia
- Bladder cancer risk (pioglitazone – debated)
- Hepatotoxicity – monitor liver function
- Macular edema (rare)
Comparative Analysis: Pioglitazone vs Rosiglitazone
| Feature | Pioglitazone | Rosiglitazone |
|---|---|---|
| Lipid profile effect | ↑ HDL, ↓ TGs | Neutral or ↑ LDL |
| Cardiovascular safety | Better profile | Higher risk (restricted use in some countries) |
| Bladder cancer concern | Reported (controversial) | Not associated |
| CYP metabolism | CYP2C8 | CYP2C8 and CYP2C9 |
| Insulin sensitivity | Improves | Improves |
Practice MCQs
Q1. TZDs act by activating which receptor?
a. GLP-1 receptor
b. Insulin receptor
c. PPAR-γ ✅
d. SGLT2
Q2. PPAR-γ activation leads to:
a. Insulin secretion
b. Increased glucose absorption
c. Increased insulin sensitivity ✅
d. Beta-cell destruction
Q3. Which of the following is TRUE about TZDs?
a. They stimulate insulin release
b. They cause hypoglycemia
c. They reduce insulin resistance ✅
d. They block glucagon receptors
Q4. Which adverse effect is associated with TZD use?
a. Hypokalemia
b. Edema ✅
c. Bradycardia
d. Renal stones
Q5. Pioglitazone affects lipid profile by:
a. Increasing LDL
b. Decreasing HDL
c. Decreasing triglycerides ✅
d. Causing hyperlipidemia
Q6. TZDs should be avoided in:
a. Liver cirrhosis
b. Congestive heart failure ✅
c. Gout
d. Hypothyroidism
Q7. What is the effect of TZDs on glucose uptake?
a. Decrease uptake
b. No effect
c. Increase via GLUT4 induction ✅
d. Block SGLT1
Q8. Rosiglitazone has been restricted in some countries due to:
a. Hepatotoxicity
b. Cardiotoxicity ✅
c. Nephrotoxicity
d. GI upset
Q9. How do TZDs affect insulin secretion?
a. Increase secretion
b. Inhibit secretion
c. No direct effect ✅
d. Destroy beta cells
Q10. TZDs are most useful in:
a. Type 1 diabetes
b. Type 2 diabetes with insulin resistance ✅
c. Gestational diabetes
d. DKA
FAQs
Q1: Can TZDs be used in type 1 diabetes?
No. They require insulin presence and are ineffective in type 1 diabetes.
Q2: Do TZDs cause hypoglycemia?
Not when used alone. However, risk increases if combined with insulin or sulfonylureas.
Q3: Are TZDs safe in heart failure?
No. They can cause fluid retention and are contraindicated in NYHA Class III/IV heart failure.
Q4: Do TZDs affect lipid profile?
Yes. Pioglitazone increases HDL and decreases triglycerides.
References
- KD Tripathi – Essentials of Medical Pharmacology
- Goodman & Gilman – The Pharmacological Basis of Therapeutics
- Review of Pharmacology – Sparsh Gupta
- ADA Guidelines
- NCBI: https://www.ncbi.nlm.nih.gov/books/NBK544294/


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com