

Table of Contents
Introduction
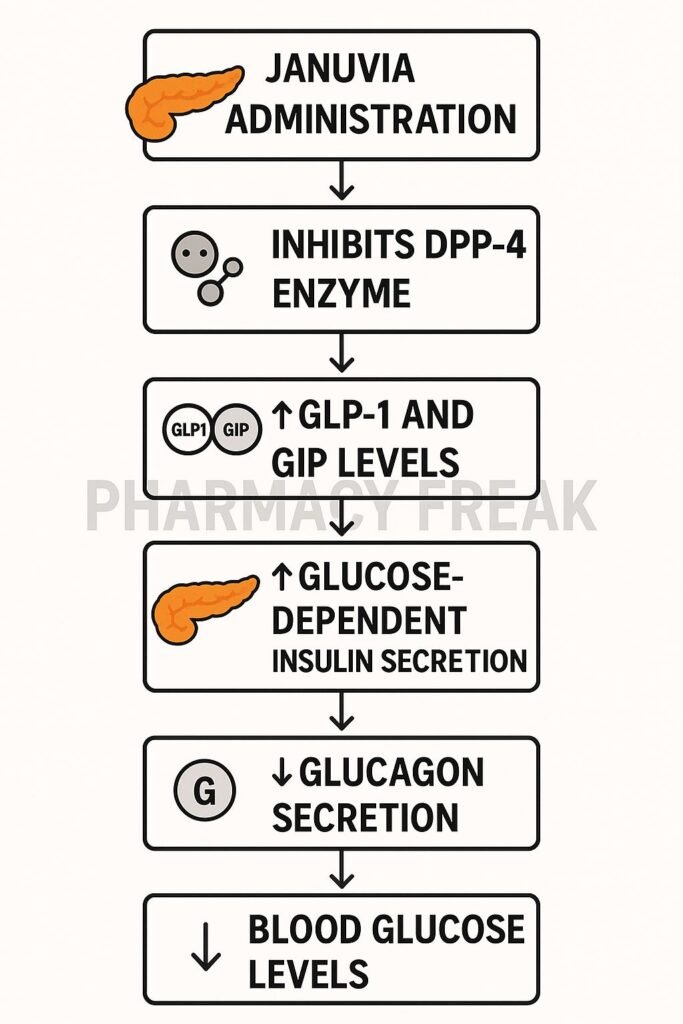
Januvia (sitagliptin) is an oral dipeptidyl peptidase‑4 (DPP‑4) inhibitor used to improve glycemic control in type 2 diabetes mellitus (T2DM). It enhances incretin levels, thereby increasing insulin secretion and lowering glucagon in a glucose-dependent manner.
Step-by-Step Mechanism of Action
- Selective inhibition of DPP‑4 enzyme
Sitagliptin irreversibly binds to and inhibits DPP‑4, preventing the degradation of incretin hormones GLP‑1 and GIP. - Increased levels of active GLP‑1 and GIP
With DPP‑4 suppressed, endogenous GLP‑1 and GIP remain active longer, boosting their physiological effects. - Enhanced glucose-dependent insulin secretion
Elevated incretins stimulate β‑cells to release insulin when blood glucose is elevated. - Suppressed glucagon secretion
Active GLP‑1 reduces α‑cell glucagon release, decreasing hepatic glucose output. - Glucose-dependent mechanism minimizes hypoglycemia risk
This pathway reduces glucose only when blood levels are high, offering a safer profile versus some other antidiabetic agents.

Pharmacokinetic Parameters
| Parameter | Value |
|---|---|
| Route | Oral (tablet) |
| Bioavailability | ~87% |
| Time to Peak (Tmax) | ~1–4 hours |
| Protein Binding | Minimal (~38%) |
| Metabolism | Excreted largely unchanged via kidneys (~79%) |
| Half-life | ~12.4 hours |
| Excretion | Primarily renal |
Clinical Uses
- Monotherapy in T2DM when diet and exercise alone are insufficient
- Combination therapy with metformin, sulfonylureas, or insulin
- Particularly useful in patients at risk of hypoglycemia or needing once-daily dosing
Adverse Effects
- Typically well tolerated
- Possible nasopharyngitis, headache, upper respiratory symptoms
- Rare: pancreatitis, hypersensitivity reactions
- Low risk of hypoglycemia when used alone
Comparative Analysis
| Drug | Incretin Mechanism | Hypoglycemia Risk | Weight Effect | Dosing |
|---|---|---|---|---|
| Sitagliptin | DPP‑4 inhibition | Low | Weight neutral | Once daily |
| Saxagliptin | DPP‑4 inhibition | Low | Weight neutral | Once daily |
| GLP‑1 agonists | GLP‑1 receptor agonism | Low–moderate | Weight loss | Daily or weekly |
MCQs
- Januvia inhibits which enzyme?
a) SGLT2 b) DPP‑4 c) α‑glucosidase d) CYP3A4
Answer: b) DPP‑4 - Inhibition increases which hormones?
a) Insulin only b) GLP‑1 and GIP c) Glucagon only d) Amylin & somatostatin
Answer: b) GLP‑1 and GIP - The glucose-lowering effect is:
a) Constant b) Glucose-dependent c) Hypoglycemia-prone d) Insulin-independent
Answer: b) Glucose-dependent - Sitagliptin is primarily excreted via:
a) Feces b) Urine c) Bile d) Sweat
Answer: b) Urine - A rare but serious side effect is:
a) Hypoglycemia b) Pancreatitis c) Hypothyroidism d) Bladder cancer
Answer: b) Pancreatitis - Protein binding is approximately:
a) 10% b) 38% c) 80% d) 99%
Answer: b) 38% - DPP‑4 inhibitors differ from GLP‑1 agonists by:
a) Oral vs injection b) Cost only c) Efficacy only d) Indication only
Answer: a) Oral vs injection - Combination with sulfonylureas increases risk of:
a) Pancreatitis b) Heart failure c) Hypoglycemia d) Weight gain
Answer: c) Hypoglycemia - Dose scheduling is:
a) Multiple times daily b) Once daily c) Every other day d) Weekly
Answer: b) Once daily - Sitagliptin therapy is least likely to cause:
a) Hypoglycemia b) Weight gain c) Nasopharyngitis d) Pancreatitis
Answer: a) Hypoglycemia - Onset of action occurs within:
a) Minutes b) Hours c) Days d) Weeks
Answer: b) Hours - Compared to saxagliptin, sitagliptin has:
a) Higher potency b) Lower potency c) Similar profile d) Different mechanism
Answer: c) Similar profile - Sitagliptin should be dose-adjusted for:
a) Liver disease b) Renal impairment c) Hypothyroidism d) Pregnancy
Answer: b) Renal impairment - Weight effect of sitagliptin is:
a) Weight gain b) Weight loss c) Weight neutral d) Unknown
Answer: c) Weight neutral - Sitagliptin carries risk of heart failure?
a) High risk b) Moderate risk c) Low risk except with saxagliptin d) No risk
Answer: c) Low risk except with saxagliptin
FAQs
1. Does sitagliptin cause weight gain?
No—it’s generally weight neutral, making it suitable for patients where weight gain is a concern.
2. When should renal function be checked?
Assess baseline renal function and adjust dose in CKD stages 3–5.
3. Is sitagliptin safe with insulin?
Yes, but monitor for hypoglycemia, especially when combined with insulin or sulfonylureas.
4. How fast does it lower blood sugar?
HbA₁c reductions typically occur within 8–12 weeks of therapy.
5. Are there cardiovascular benefits?
Neutral cardiovascular outcomes have been observed; it’s safe but not proven to reduce CV events.
References
- Goodman & Gilman’s The Pharmacological Basis of Therapeutics, 13th Edition
- KD Tripathi. Essentials of Medical Pharmacology, 8th Edition
- DrugBank: Sitagliptin pharmacology summary
- StatPearls: Sitagliptin and other DPP‑4 inhibitors
- PubMed review: Cardiovascular safety of sitagliptin


I am pursuing MBA in pharmaceutical management from NIPER Hyderabad with a strong academic record and proven success in national-level pharmacy entrance exams. I secured AIR 61 in NIPER 2024 (MS/M.Pharm) and AIR 27 in NIPER MBA, along with AIR 147 in GPAT 2024 and AIR 907 in GPAT 2023. I also achieved AIR 6 in AIIMS CRE-2025 for Drug Store Keeper and was selected as a Pharmacist (AIR 61) for ESIC. Additionally, I was the Runner-Up in Round 2 of the EY Case Study Competition.
At PharmacyFreak.com, I aim to guide future pharmacists through expert content, exam strategies, and insightful resources based on real experience and academic excellence.
Mail- harsh@pharmacyfreak.com