High cholesterol and triglyceride levels are major risk factors for heart disease and stroke. Hypolipidemic drugs help reduce lipid levels in the blood and are crucial in preventing atherosclerosis and cardiovascular complications.
In this blog by Pharmacy Freak, we’ll explain the classification, mechanisms, and uses of hypolipidemic drugs, with references from Sparsh Gupta, K.D. Tripathi, and Goodman & Gilman’s — ideal for medical and pharmacy students.
Table of Contents
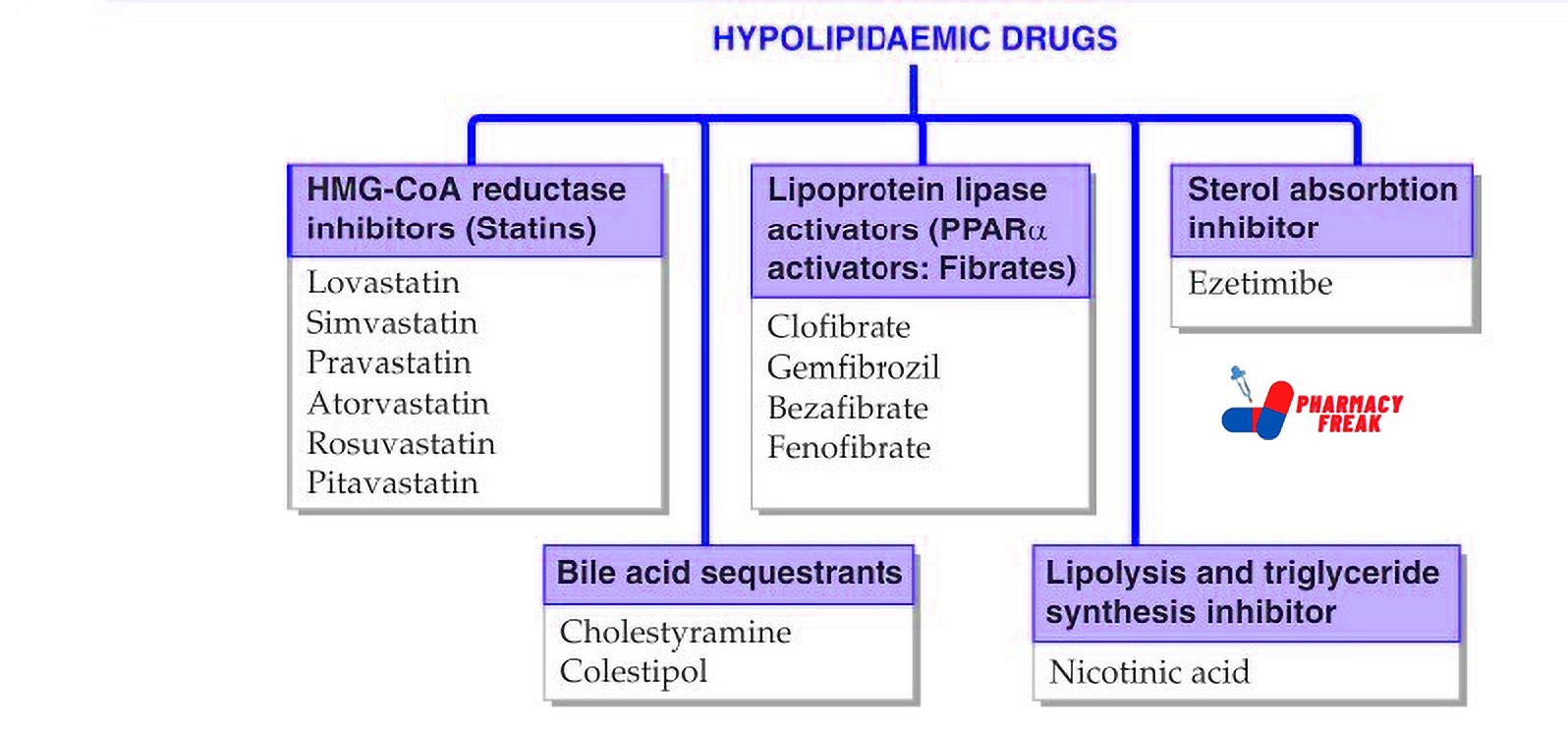
Hypolipidemic Drugs Classification (KD Tripathi)
- HMG-CoA reductase inhibitors (Statins): Lovastatin, Simvastatin, Pravastatin, Atorvastatin, Rosuvastatin, Pitavastatin
- Lipoprotein lipase activators (PPARα activators: Fibrates): Clofibrate, Gemfibrozil, Bezafibrate, Fenofibrate
- Sterol absorption inhibitor: Ezetimibe
- Bile acid sequestrants: Cholestyramine, Colestipol
- Lipolysis and triglyceride synthesis inhibitor: Nicotinic acid
Hypolipidemic Drugs Classification (General Classification)
HMG-CoA Reductase Inhibitors (Statins)
Mechanism: Inhibit HMG-CoA reductase, reducing hepatic cholesterol synthesis.
Drugs: Atorvastatin, Rosuvastatin, Simvastatin, Pravastatin, Lovastatin
Statins are the most effective class for lowering LDL cholesterol.
- Fibrates
Mechanism: Activate PPAR-α, increasing lipoprotein lipase activity and reducing triglyceride levels.
Drugs: Fenofibrate, Gemfibrozil - Nicotinic Acid (Niacin)
Mechanism: Inhibits VLDL synthesis and decreases HDL catabolism.
Used in combined hyperlipidemia. - Bile Acid Sequestrants
Mechanism: Bind bile acids in the intestine, forcing the liver to use cholesterol to make more bile acids.
Drugs: Cholestyramine, Colestipol - Cholesterol Absorption Inhibitors
Mechanism: Inhibit NPC1L1 transporter in the intestine to reduce cholesterol absorption.
Drug: Ezetimibe - PCSK9 Inhibitors
Mechanism: Monoclonal antibodies that increase LDL receptor recycling and reduce plasma LDL levels.
Drugs: Alirocumab, Evolocumab - Omega-3 Fatty Acids
Mechanism: Reduce hepatic VLDL and triglyceride synthesis.
Drugs: EPA, DHA, Icosapent ethyl - Newer Agents
- Bempedoic acid – Inhibits ATP citrate lyase.
- Inclisiran – siRNA against PCSK9 gene.
- Lomitapide, Mipomersen – For familial hypercholesterolemia.
Uses
Hypolipidemic drugs are used in the treatment and prevention of:
- Hypercholesterolemia
- Hypertriglyceridemia
- Mixed dyslipidemia
- Familial lipid disorders
- Atherosclerosis and coronary artery disease
- Prevention of myocardial infarction and stroke
Drug of Choice Highlights
Based on current standard textbooks, the following are the recommended drugs of choice:
- Hypercholesterolemia – Atorvastatin or Rosuvastatin
- Hypertriglyceridemia – Fenofibrate
- Mixed hyperlipidemia – Statins with Fibrate (with monitoring)
- Statin intolerance – Ezetimibe or PCSK9 inhibitors
- Familial hypercholesterolemia – Evolocumab or Lomitapide
- Atherosclerotic prevention – High-intensity statin (Atorvastatin or Rosuvastatin)
Side Effects
- Statins – Myopathy, hepatotoxicity, new-onset diabetes in some cases
- Fibrates – Gallstones, myopathy, especially when combined with statins
- Niacin – Flushing, hyperglycemia, hepatotoxicity, hyperuricemia
- Bile acid resins – Constipation, bloating, interference with absorption of fat-soluble vitamins
- Ezetimibe – Generally well tolerated; occasional GI upset
- PCSK9 inhibitors – Injection site reactions; high cost
- Omega-3 fatty acids – Fishy aftertaste, GI discomfort
Updated Clinical Pearls
- Statins not only lower LDL but also reduce cardiovascular events and mortality.
- Always monitor liver enzymes (LFT) and muscle enzyme (CK) when using statins or fibrates.
- Ezetimibe is the preferred non-statin agent to be combined with statins when LDL goals are not achieved.
- PCSK9 inhibitors are highly effective in lowering LDL, especially in familial hypercholesterolemia or statin intolerance, though cost is a barrier.
- Icosapent ethyl has shown cardiovascular benefit in patients with elevated triglycerides despite statin use.
- Bempedoic acid is a promising new oral agent with fewer muscle-related side effects compared to statins.
References
- Tripathi KD. Essentials of Medical Pharmacology. 7th ed. New Delhi: Jaypee Brothers Medical Publishers; 2013. p. 624–633.
- Gupta S, Garg A. Review of Pharmacology. 15th ed. New Delhi: Jaypee Brothers Medical Publishers; 2023. p. 261–265.
- Brunton LL, Chabner BA, Knollmann BC, editors. Goodman and Gilman’s The Pharmacological Basis of Therapeutics. 12th ed. New York: McGraw-Hill Education; 2011. p. 877–884.
Related Links


