Table of Contents
Introduction
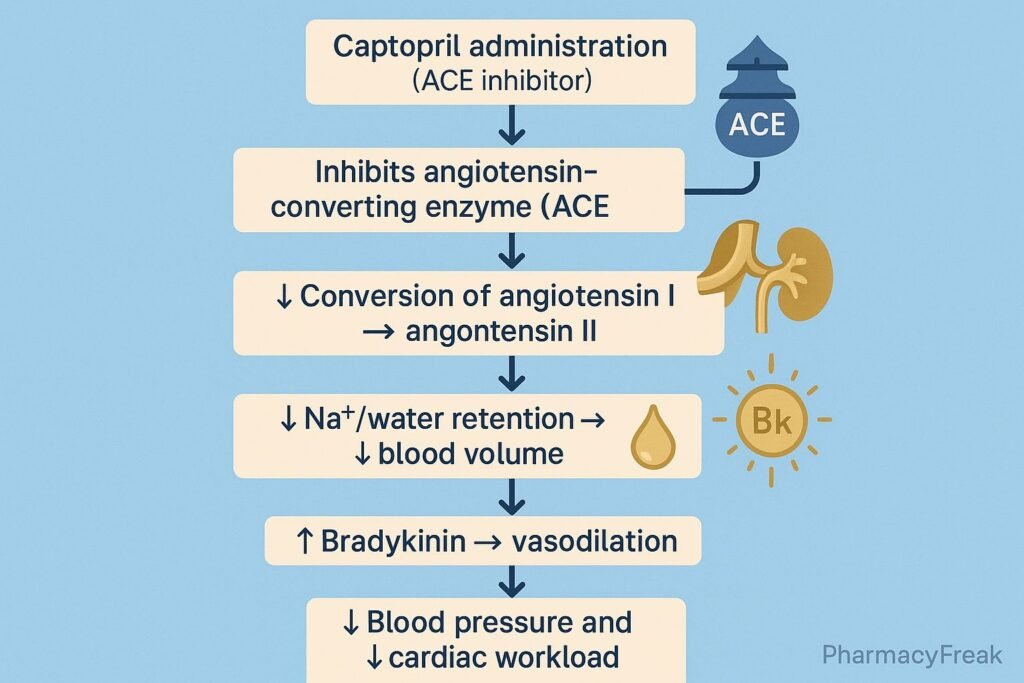
Captopril is a first-generation angiotensin-converting enzyme (ACE) inhibitor used in the management of hypertension, heart failure, diabetic nephropathy, and post-myocardial infarction ventricular remodeling. It was the first ACE inhibitor developed and remains clinically relevant, especially for acute blood pressure control due to its rapid onset.
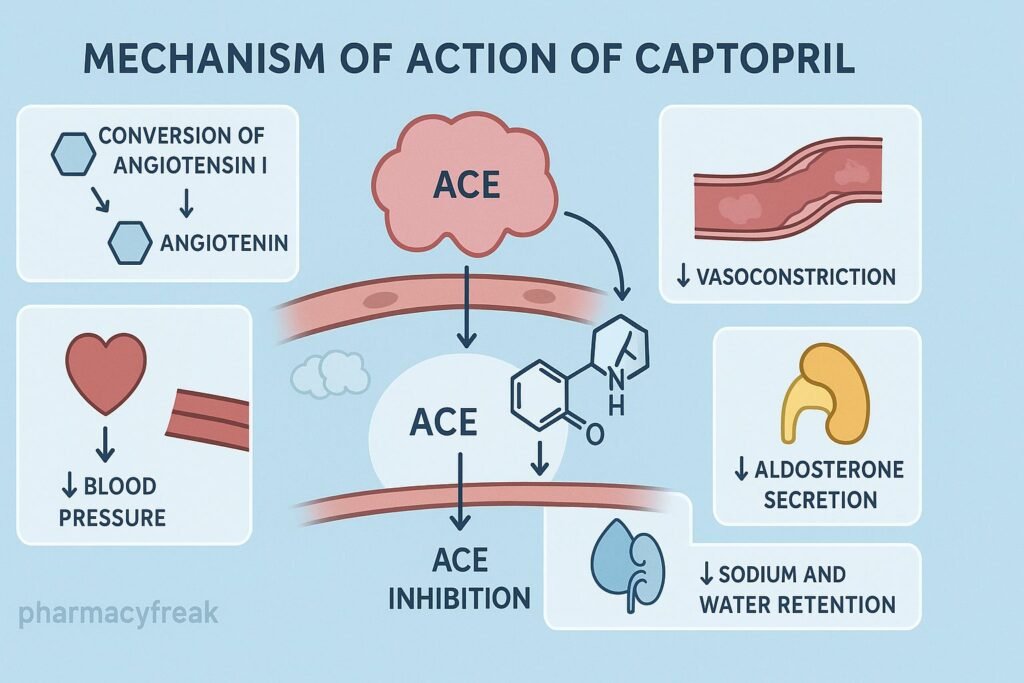
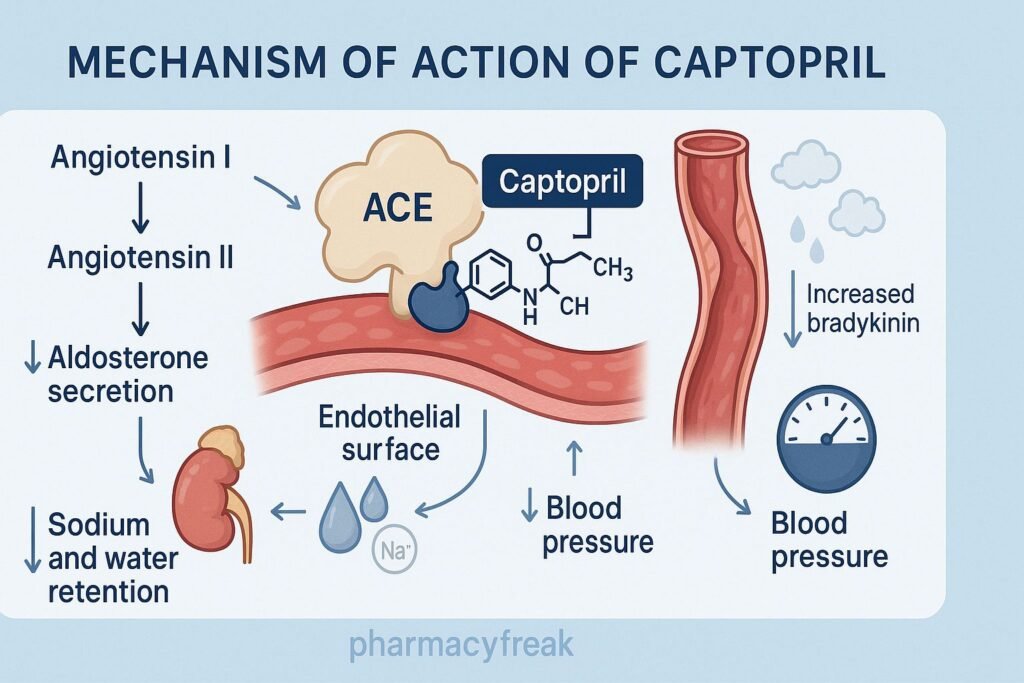
The Mechanism of Action of Captopril is based on inhibition of ACE, leading to decreased angiotensin II formation, reduced aldosterone secretion, and increased bradykinin levels, resulting in vasodilation, natriuresis, and reduced cardiovascular remodeling.

Mechanism of Action (Step-wise)
1. Inhibition of ACE (Angiotensin-Converting Enzyme) – Primary Mechanism
Captopril directly inhibits ACE, preventing conversion of:
Angiotensin I → Angiotensin II
Effects of ↓ Angiotensin II:
- ↓ Arteriolar vasoconstriction
- ↓ Aldosterone secretion
- ↓ Sodium and water retention
- ↓ Sympathetic activity
- ↓ Vasopressin release
Result: Decreased systemic vascular resistance and blood pressure.
2. Increased Bradykinin Levels
ACE also breaks down bradykinin, a potent vasodilator.
Captopril ↓ Bradykinin degradation →
- ↑ Nitric oxide (NO)
- ↑ Prostaglandins
- ↑ Vasodilation
This contributes to antihypertensive action but also causes dry cough and angioedema.
3. Reduced Aldosterone Secretion
Less angiotensin II → less aldosterone.
Effects:
- ↓ Sodium reabsorption
- ↓ Water retention
- ↓ Potassium excretion → may cause hyperkalemia
4. Decreased Preload and Afterload
Due to venous and arterial dilation, captopril:
- ↓ Preload (improves heart failure)
- ↓ Afterload (reduces cardiac workload)
5. Reduced Cardiac and Vascular Remodeling
Angiotensin II promotes hypertrophy and fibrosis.
Captopril reduces:
- Left ventricular hypertrophy
- Ventricular dilation post-MI
- Progression of diabetic nephropathy
- Glomerular hypertension and proteinuria
6. Summary of Mechanism
| Mechanism | Effect |
|---|---|
| ACE inhibition | ↓ Ang II → vasodilation |
| ↓ Aldosterone | ↓ Na⁺/H₂O retention |
| ↑ Bradykinin | NO & PGI₂-mediated vasodilation |
| ↓ Sympathetic tone | Lower BP |
| ↓ Remodeling | Cardioprotection |
Pharmacokinetics
- Class: Sulfhydryl-containing ACE inhibitor
- Route: Oral
- Onset: 15–30 minutes
- Duration: 6–12 hours
- Bioavailability: 70%
- Metabolism: Minimal
- Excretion: Renal (requires dose adjustment)
Clinical Uses
- Hypertension
- Heart failure (adjunct)
- Diabetic nephropathy
- Post-MI ventricular remodeling prevention
- Hypertensive emergency (oral, short-term)
Adverse Effects
- Dry cough
- Angioedema
- Hyperkalemia
- Hypotension
- Renal impairment (especially in bilateral renal artery stenosis)
- Skin rash and taste disturbances (due to sulfhydryl group)
Contraindications
- Pregnancy (teratogenic)
- Bilateral renal artery stenosis
- History of angioedema
- Hyperkalemia
- Severe renal impairment
Comparative Analysis
| Feature | Captopril | Enalapril | Lisinopril |
|---|---|---|---|
| Onset | Rapid | Slower | Slow |
| Duration | Short | Intermediate | Long |
| Dosing | 2–3 times daily | 1–2 times daily | Once daily |
| Special | Sulfhydryl group | Prodrug | Not a prodrug |
MCQs
1. Captopril lowers blood pressure primarily by inhibiting:
a) Renin
b) ACE
c) Aldosterone receptors
d) Beta receptors
Answer: b) ACE
2. Increased bradykinin due to captopril leads to:
a) Bronchoconstriction
b) Vasodilation
c) Sodium retention
d) Tachycardia
Answer: b) Vasodilation
3. A common adverse effect of captopril is:
a) Hypernatremia
b) Dry cough
c) Hypokalemia
d) Constipation
Answer: b) Dry cough
4. Captopril is contraindicated in:
a) Diabetes
b) Bilateral renal artery stenosis
c) Liver failure
d) Asthma
Answer: b) Bilateral renal artery stenosis
5. Which electrolyte imbalance may occur?
a) Hypocalcemia
b) Hyperkalemia
c) Hypermagnesemia
d) Hypophosphatemia
Answer: b) Hyperkalemia
FAQs
Q1. Why does captopril cause cough?
Due to increased bradykinin levels in the lungs.
Q2. Can captopril cause hyperkalemia?
Yes—due to decreased aldosterone activity.
Q3. Is captopril safe in pregnancy?
No—ACE inhibitors are teratogenic.
Q4. Why is captopril useful post-MI?
Prevents ventricular remodeling.
Q5. Does food affect captopril absorption?
Yes—food decreases its absorption.
References
Goodman & Gilman’s Pharmacological Basis of Therapeutics
https://accesspharmacy.mhmedical.com/book.aspx?bookid=2189
Katzung: Basic and Clinical Pharmacology
https://accessmedicine.mhmedical.com/book.aspx?bookid=2464
Tripathi: Essentials of Medical Pharmacology
https://jaypeebrothers.com/
Harrison’s Principles of Internal Medicine
https://accessmedicine.mhmedical.com/book.aspx?bookid=2129


